Abdelrazek Ali Yasmin, Nour El-Deen Nehad El-Sayed, Elshahed Ghada Samir
Congenital and Structural Heart Diseases Unit, Cardiology Department, Ain Shams University, El Cairo, Egipto Congenital and Structural Heart Diseases Unit Cardiology Department Ain Shams University El Cairo Egipto.
REC Interv Cardiol. 2024 Oct 16;6(4):296-304. doi: 10.24875/RECIC.M24000475. eCollection 2024 Oct-Dec.
The bidirectional Glenn shunt (BDG) is an essential step in the repair of a physiologically single-ventricle heart. BDG increases pulmonary blood flow, allows growth of the pulmonary arteries, and improves SaO. The procedure also allows unloading of ventricular volume, thereby improving survival. Our aim was to register all patients who developed collaterals following BDG, document the management methods used, and assess their impact.
We included 56 patients who underwent BDG procedures at a median age of 2.08 (1-3) years. After BDG, peripheral pulmonary stenting was used in 2 patients. Symptomatic hyperviscosity was present in 10 patients (17.86%), who underwent venesection. BDG was unsuccessful in 2 patients. Venovenous collaterals were observed in 41 patients (73.2%), and aortopulmonary collaterals in 37 (66.1%).
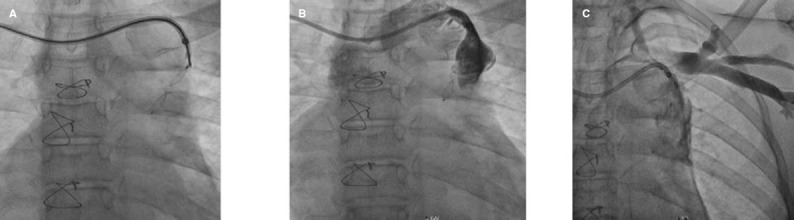
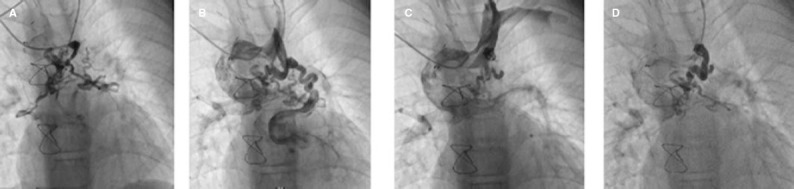
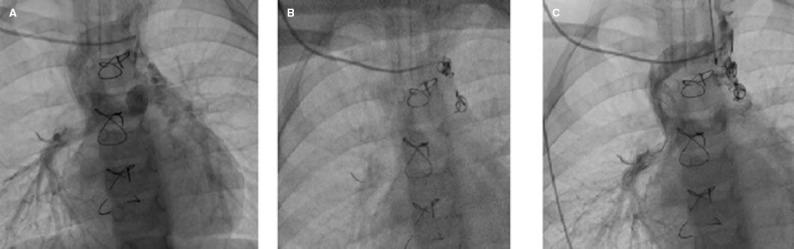
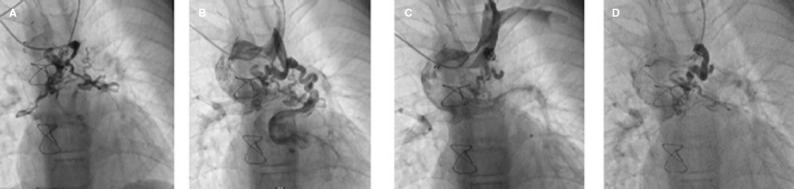
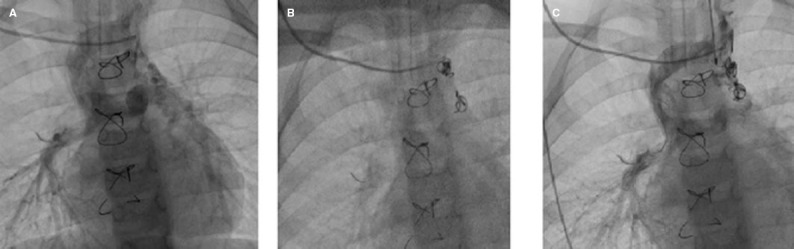
Hematocrit levels were significantly higher in patients with venovenous collaterals (50.00 ± 8.76) than in those without ( = .031). Mean pulmonary artery pressure was also significantly higher in patients with venovenous collaterals (15 [12-18] mmHg; = .025). One patient had undergone successful closure of venovenous collaterals to epicardial veins and abdominal veins 3 years previously. Seven patients underwent transcatheter closure (TCC) of collaterals. Of these, 4 patients underwent TCC of venovenous collaterals to left and right pulmonary veins; 1 patient underwent closure of an aortopulmonary collateral; 1 patient underwent a failed attempt at venovenous collateral closure that was complicated by an ischemic stroke; and 1 patient had localized extravasation upon separation of the cable. A highly statistically significant increase in SaO was observed after TCC of venovenous collaterals (69.83 ± 10.91 vs 82.83 ± 9.87; = .008).
TCC of collaterals is a technically demanding but effective management strategy following BDG to improve patients' SaO and quality of life. Awareness of possible complications and their effective management is crucial.
双向格林分流术(BDG)是生理性单心室心脏修复的关键步骤。BDG可增加肺血流量,促进肺动脉生长,并提高动脉血氧饱和度(SaO)。该手术还能减轻心室容量负荷,从而提高生存率。我们的目的是登记所有在BDG术后出现侧支循环的患者,记录所采用的治疗方法,并评估其影响。
我们纳入了56例接受BDG手术的患者,中位年龄为2.08(1 - 3)岁。BDG术后,2例患者接受了外周肺动脉支架置入术。10例患者(17.86%)出现有症状的高黏滞血症,接受了静脉切开术。2例患者BDG手术失败。41例患者(73.2%)观察到腔静脉侧支循环,37例患者(66.1%)观察到主肺动脉侧支循环。
有腔静脉侧支循环的患者血细胞比容水平(50.00 ± 8.76)显著高于无腔静脉侧支循环的患者(P = .031)。有腔静脉侧支循环的患者平均肺动脉压也显著更高(15 [12 - 18] mmHg;P = .025)。1例患者3年前成功将腔静脉侧支循环闭合至心外膜静脉和腹壁静脉。7例患者接受了侧支循环的经导管封堵术(TCC)。其中,4例患者对腔静脉至左右肺静脉的侧支循环进行了TCC;1例患者对主肺动脉侧支循环进行了封堵;1例患者腔静脉侧支循环封堵尝试失败,并并发缺血性卒中;1例患者在分离导管时出现局部渗漏。腔静脉侧支循环TCC术后观察到SaO有高度统计学意义的升高(69.83 ± 10.91 vs 82.83 ± 9.87;P = .008)。
侧支循环的TCC是BDG术后一种技术要求高但有效的治疗策略,可改善患者的SaO和生活质量。认识到可能的并发症并进行有效管理至关重要。