Gupta Aditya K, Nguyen Hien C, Liddy Amanda, Economopoulos Vasiliki, Wang Tong
Division of Dermatology, Department of Medicine, Temerty Faculty of Medicine, University of Toronto, Toronto, ON M5S 3H2, Canada.
Mediprobe Research Inc., London, ON N5X 2P1, Canada.
Antibiotics (Basel). 2025 May 7;14(5):472. doi: 10.3390/antibiotics14050472.
BACKGROUND/OBJECTIVES: Terbinafine has been the gold standard for the management of superficial fungal infections. The etiological agent generally is (); however, there has been increased reporting of a new terbinafine-resistant strain of the ( ITS genotype VIII otherwise known as ). Here, we review the epidemiology, clinical features, diagnosis, and treatment of and infections.
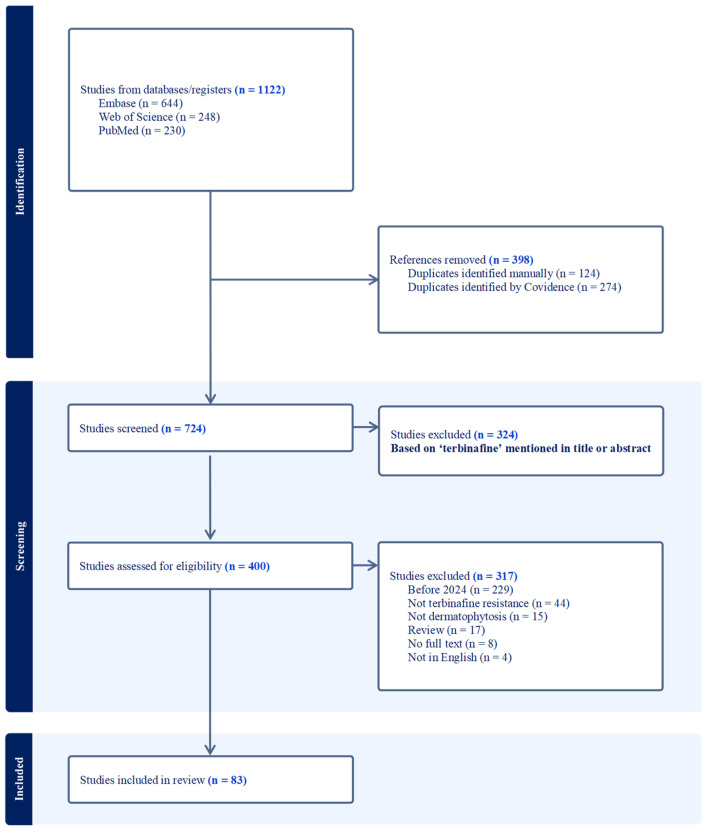
We conducted a systematic literature search using PubMed, Embase (Ovid), and Web of Science, resulting in 83 qualified studies with data summarized for clinical features, antifungal susceptibility, and terbinafine resistance mechanisms and mutations.
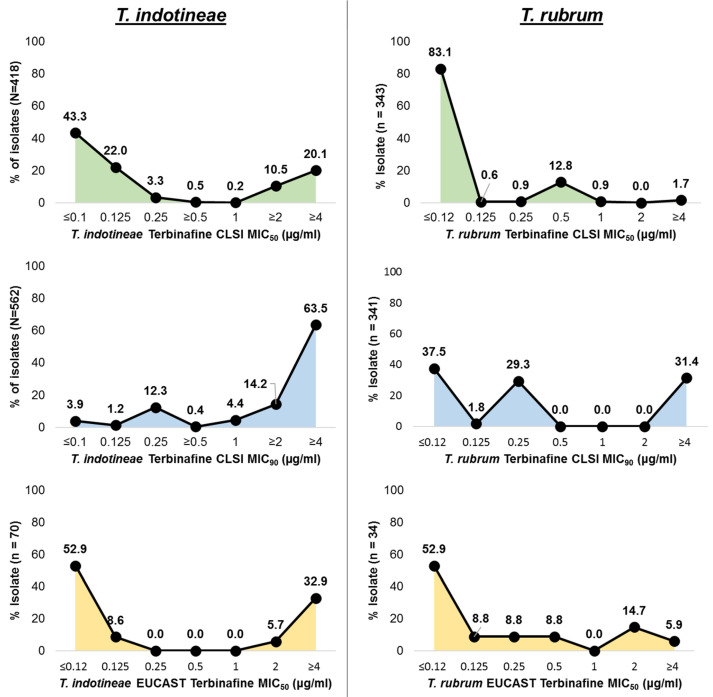
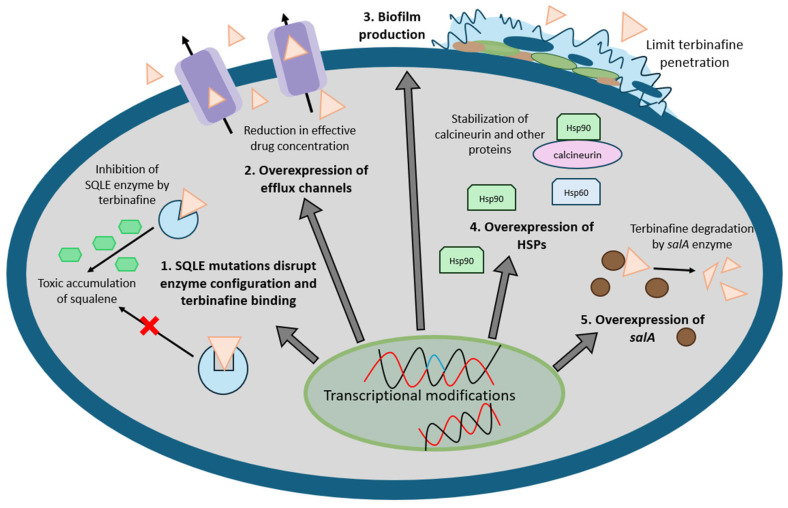
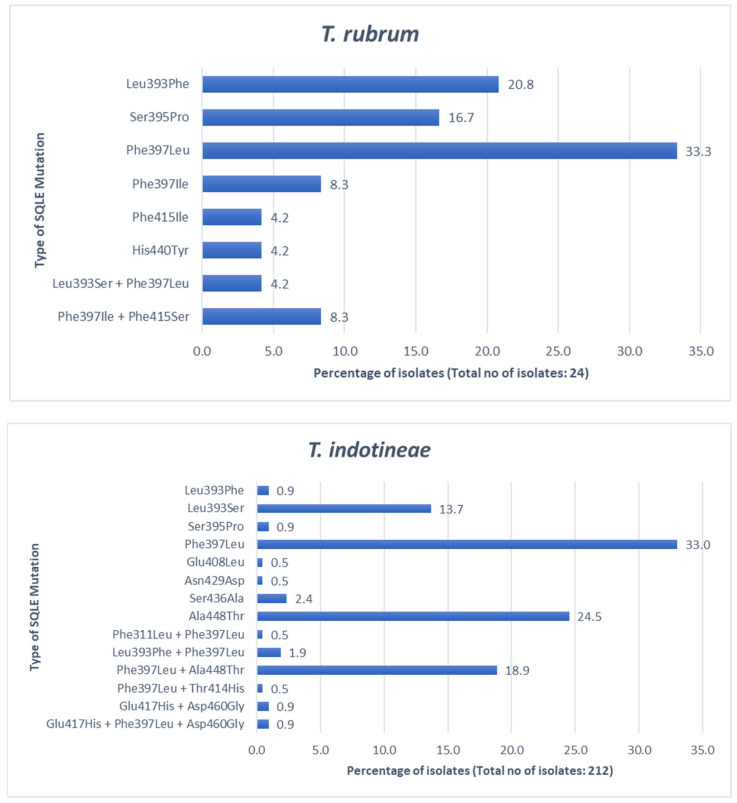
Dermatophytosis is most commonly caused by ; however, in certain parts of the world, especially in the Indian subcontinent, infections have been reported more frequently. The majority of isolates remain susceptible to terbinafine (over 60% of isolates show MIC and MIC < 0.5 µg/mL). In contrast, for , 30% of isolates exhibit MIC ≥ 0.5 µg/mL and 80% exhibit MIC ≥ 0.5 µg/mL. Frequently detected squalene epoxidase () mutations in are Phe397Leu/Ile (41.6%) and Leu393Phe (20.8%); in , these include Phe397Leu (33.0%) and Ala448Thr (24.5%). Other potential terbinafine resistance mechanisms in and are discussed.
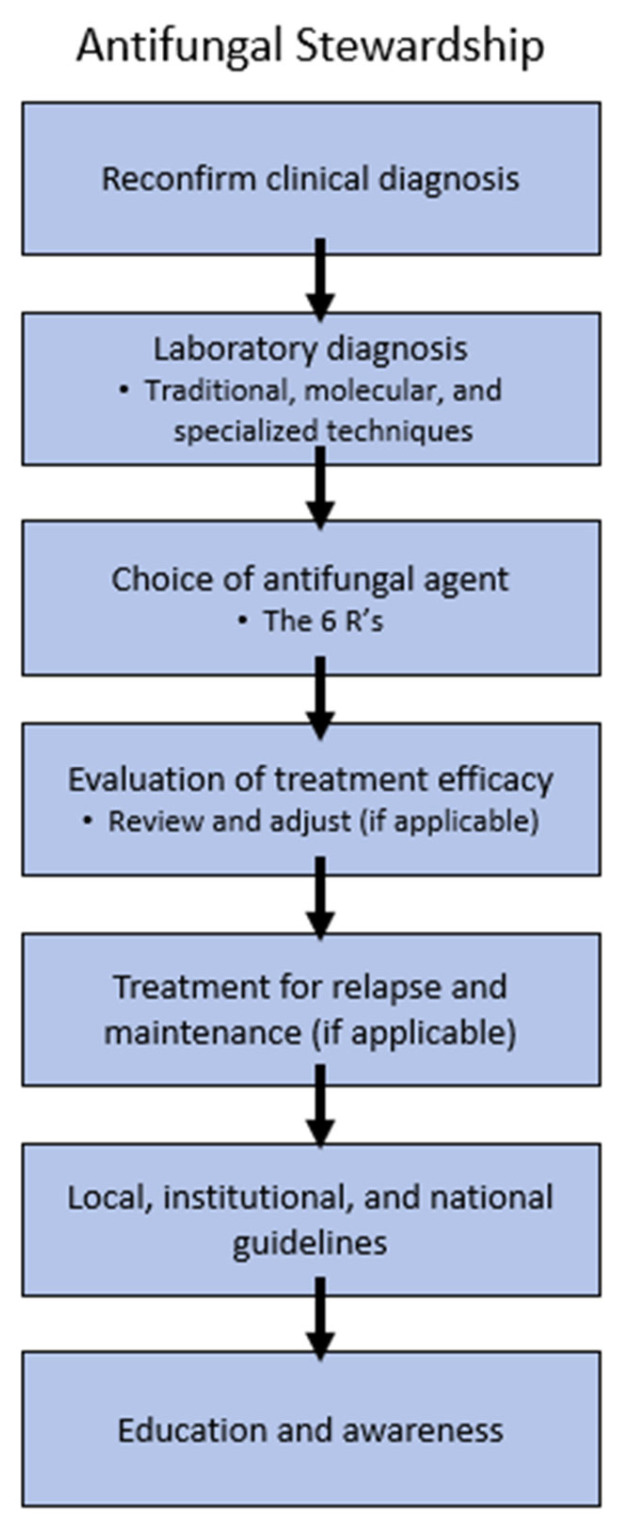
generally remain susceptible in vitro to terbinafine in contrast to . The essential components of an effective antifungal stewardship emphasize accurate clinical and laboratory diagnosis, susceptibility testing, and appropriate antifungal therapy selection with a multidisciplinary approach.
背景/目的:特比萘芬一直是治疗浅表真菌感染的金标准。病原体通常是();然而,一种新的对特比萘芬耐药的(ITS基因型VIII,也称为)菌株的报告有所增加。在此,我们综述了()和()感染的流行病学、临床特征、诊断和治疗。
我们使用PubMed、Embase(Ovid)和Web of Science进行了系统的文献检索,得到83项合格研究,总结了临床特征、抗真菌药敏性、特比萘芬耐药机制和突变的数据。
皮肤癣菌病最常见的病因是();然而,在世界某些地区,特别是印度次大陆,()感染的报告更为频繁。大多数()分离株对特比萘芬仍敏感(超过60%的分离株显示MIC且MIC<0.5μg/mL)。相比之下,对于(),30%的分离株MIC≥0.5μg/mL,80%的分离株MIC≥0.5μg/mL。在()中经常检测到的角鲨烯环氧化酶()突变是Phe397Leu/Ile(41.6%)和Leu393Phe(20.8%);在()中,这些包括Phe397Leu(33.0%)和Ala448Thr(24.5%)。还讨论了()和()中其他潜在的特比萘芬耐药机制。
与()相比,()在体外通常对特比萘芬敏感。有效的抗真菌管理的基本要素强调准确的临床和实验室诊断、药敏试验以及采用多学科方法选择合适的抗真菌治疗。