Hao Shiying, Velásquez Esther E, Pearson William S, Hoover Karen W, Zhu Weiming, Rochlin Ilia, Vala Ayin, Chu Isabella, Phillips Robert L, Rehkopf David H, Kamdar Neil
Center for Population Health Sciences, School of Medicine, Stanford University, Palo Alto, California, United States of America.
Division of STD Prevention, Centers for Disease Control and Prevention, Atlanta, GeorgiaUnited States of America.
PLoS One. 2025 Jun 2;20(6):e0325097. doi: 10.1371/journal.pone.0325097. eCollection 2025.
Early identification and treatment of sexually transmitted infections (STIs) is critical to improve patient outcomes. Barriers to healthcare seeking are potentially exacerbated by COVID-19. This study examined trends in STI testing and positivity from 2019 to 2021 in primary care in the United States.
This is a retrospective study using the PRIME Registry, a national primary care EHR registry, from January 1, 2019-December 31, 2021. We calculated age-standardized monthly and annual testing rates for chlamydia, gonorrhea, syphilis, and human immunodeficiency virus stratified by gender and race/ethnicity. We also generated quarterly and annual rates for test positivity. Chi-square tests and 95% confidence intervals were used for comparison. 753 practices and 4,410,609 patients were included, with 180,558 having STI tests.
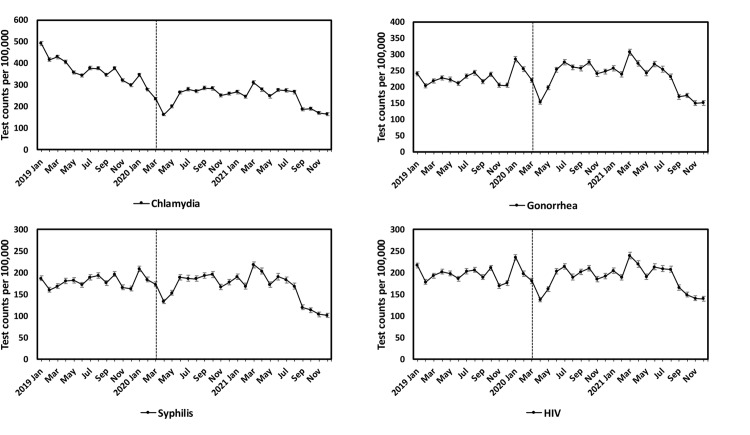
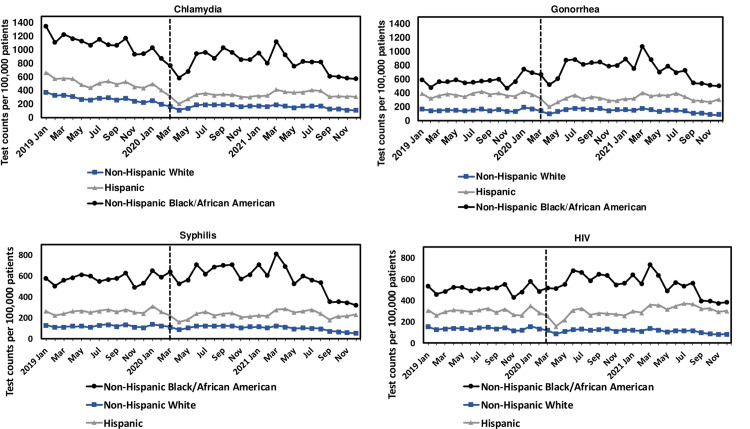
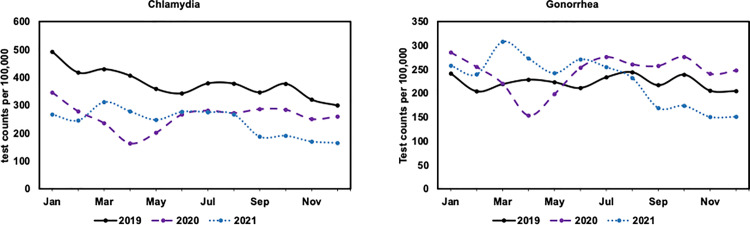
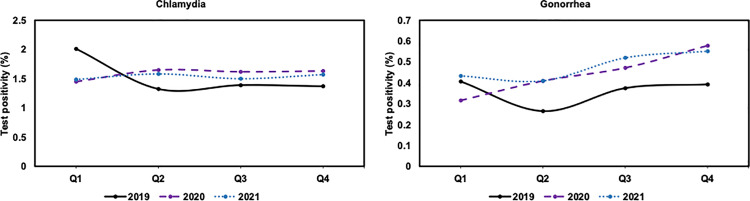
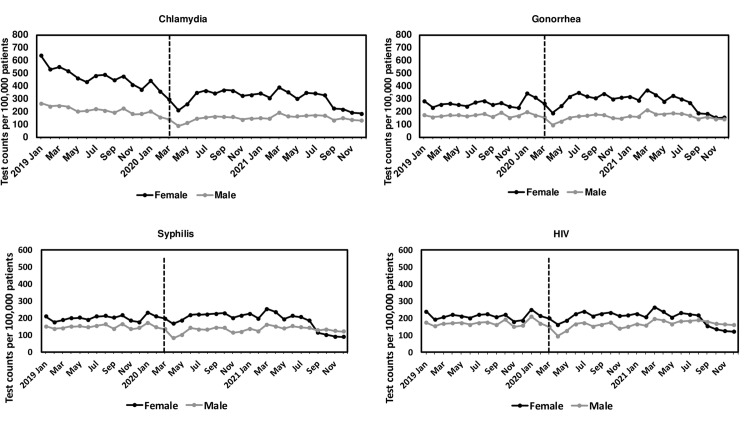
We observed a substantial decline in testing rates for STIs from March-April 2020 (31% for chlamydia, 30% for gonorrhea, 23% for syphilis, 24% for HIV), followed by a rapid increase in May-June 2020 (64% for chlamydia, 65% for gonorrhea, 32% for syphilis, 48% for HIV). Testing rates per 100,000 decreased from 2019 to 2021 for chlamydia (3,592 vs 2,355 vs 2,181) while increased for gonorrhea in 2020 (2,129 vs 2,207 vs 2,057). STI testing rates from 2019 to 2021 for females and non-Hispanic Black or African American patients were higher than other groups. An increase in test positivity from 2019 to 2021 was observed for gonorrhea (0.4% vs 0.4% vs 0.5%) but no significant change for chlamydia (1.5% vs 1.6% vs 1.5%).
Testing rates for STIs substantially dropped during stay-at-home orders early in the pandemic and recovered after these were relaxed. Gender and race/ethnicity STI testing differences may reflect primary care's prioritization of higher risk populations. This study emphasizes the role of primary care EHR data in monitoring and an opportunity for closer collaboration with public health agencies.
性传播感染(STIs)的早期识别和治疗对于改善患者预后至关重要。新冠疫情可能加剧了寻求医疗服务的障碍。本研究调查了2019年至2021年美国初级保健中性传播感染检测及阳性率的趋势。
这是一项回顾性研究,使用了PRIME注册系统,这是一个全国性的初级保健电子健康记录注册系统,时间跨度为2019年1月1日至2021年12月31日。我们计算了按性别和种族/民族分层的衣原体、淋病、梅毒和人类免疫缺陷病毒的年龄标准化月度和年度检测率。我们还生成了检测阳性率的季度和年度数据。采用卡方检验和95%置信区间进行比较。纳入了753家医疗机构和4410609名患者,其中180558人进行了性传播感染检测。
我们观察到2020年3月至4月性传播感染检测率大幅下降(衣原体下降31%,淋病下降30%,梅毒下降23%,艾滋病毒下降24%),随后在2020年5月至6月迅速上升(衣原体上升64%,淋病上升65%,梅毒上升32%,艾滋病毒上升48%)。衣原体每10万人的检测率从2019年到2021年有所下降(分别为3592、2355、2181),而淋病在2020年有所上升(分别为2129、2207、2057)。2019年至2021年,女性以及非西班牙裔黑人或非裔美国患者的性传播感染检测率高于其他群体。2019年至2021年,淋病的检测阳性率有所上升(分别为0.4%、0.4%、0.5%),而衣原体则无显著变化(分别为1.5%、1.6%、1.5%)。
在疫情早期居家令期间,性传播感染检测率大幅下降,在限制放宽后有所恢复。性别和种族/民族在性传播感染检测方面的差异可能反映了初级保健对高风险人群的优先关注。本研究强调了初级保健电子健康记录数据在监测中的作用,以及与公共卫生机构加强合作的机会。