Kurniansyah Nuzulul, Strausz Satu J, Chittoor Geetha, Gupta Shreyash, Justice Anne E, Hrytsenko Yana, Keenan Brendan T, Cade Brian E, Spitzer Brian W, Wang Heming, Huffman Jennifer, Moll Matthew R, Haring Bernhard, Jung Su Yon, Raffield Laura M, Kaplan Robert, Rotter Jerome I, Rich Stephen S, Gharib Sina A, Bartz Traci M, Liu Peter Y, Chen Han, Fornage Myriam, Hou Lifang, Levy Daniel, Morrison Alanna C, Ochs-Balcom Heather M, Psaty Bruce M, Wilson Peter W F, Cho Kelly, Pack Allan I, Ollila Hanna M, Redline Susan, Gottlieb Daniel J, Sofer Tamar
VA Boston Healthcare System, Boston, MA, USA; Division of Sleep and Circadian Disorders, Department of Medicine, Brigham and Women's Hospital, Boston, MA, USA; Department of Bioinformatics, Boston University, Boston, MA, USA.
Institute for Molecular Medicine Finland, Helsinki Institute of Life Science, University of Helsinki, Helsinki, Finland; Department of Genetics, Stanford University School of Medicine, Stanford, CA, USA; Department of Oral and Maxillofacial Diseases, Helsinki University Hospital, Helsinki, Finland; Department of Cleft Palate and Craniofacial Center, University of Helsinki and Helsinki University Hospital, Helsinki, Finland; Orthodontics, Department of Oral and Maxillofacial Diseases, Clinicum, Faculty of Medicine, University of Helsinki, Helsinki, Finland.
EBioMedicine. 2025 Jun 4;117:105790. doi: 10.1016/j.ebiom.2025.105790.
Obstructive sleep apnoea (OSA) is a common chronic condition, with obesity its strongest risk factor. Polygenic scores (PGSs) summarise the genetic liability to phenotype and can provide insights into relationships between phenotypes. Recently, large datasets that include genetic data and OSA status became available, providing an opportunity to utilise PGS approaches to study the genetic relationship between OSA and other phenotypes, while differentiating OSA-specific from obesity-specific genetic factors.
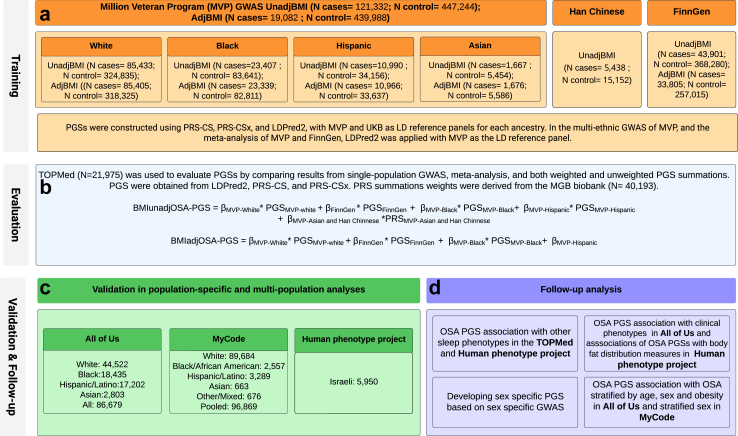
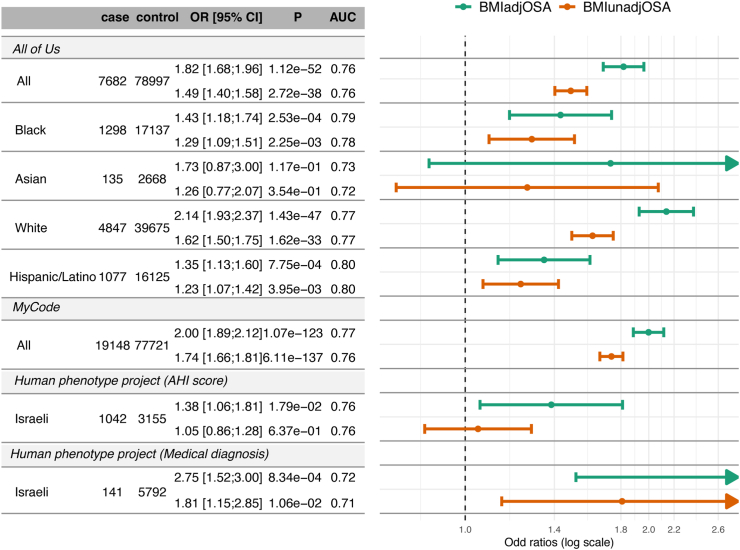
Using race/ethnic diverse samples from over 1.2 million individuals from the Million Veteran Program, FinnGen, TOPMed, All of Us (AoU), Geisinger's MyCode, MGB Biobank, and the Human Phenotype Project, we developed and assessed PGSs for OSA, both without (BMIunadjOSA-PGS) and with adjustment for the genetic contributions of BMI (BMIadjOSA-PGS).
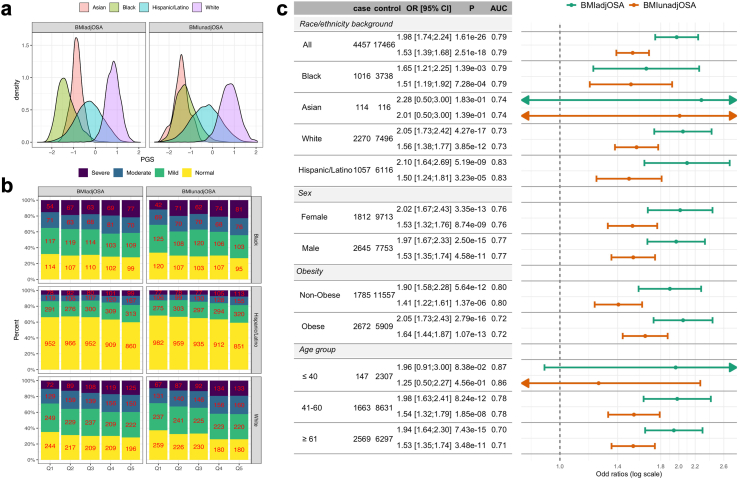
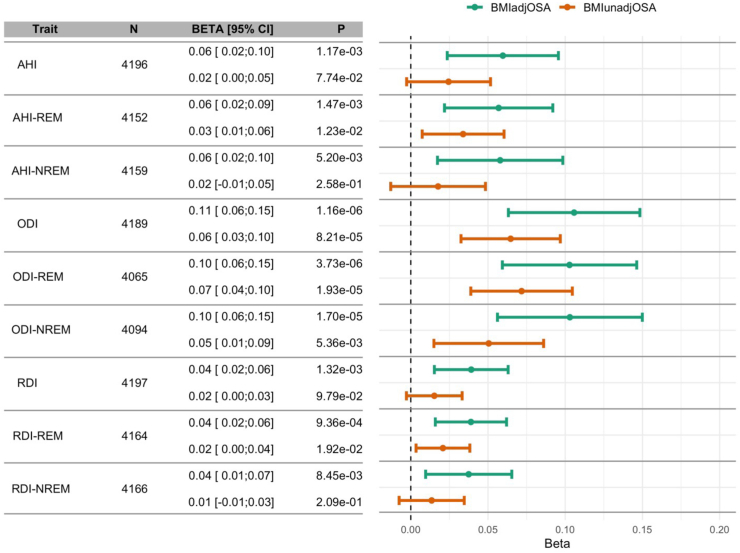
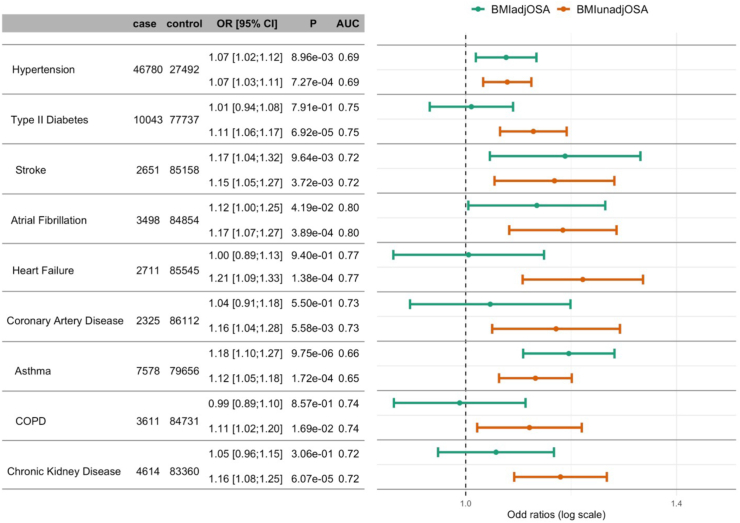
Adjusted odds ratios (ORs) for OSA per 1 standard deviation of the PGSs ranged from 1.38 to 2.75. The associations of BMIadjOSA- and BMIunadjOSA-PGSs with CVD outcomes in AoU shared both common and distinct patterns. Only BMIunadjOSA-PGS was associated with type 2 diabetes, heart failure, and coronary artery disease, while both BMIadjOSA- and BMIunadjOSA-PGSs were associated with hypertension and stroke. Sex stratified analyses revealed that BMIadjOSA-PGS association with hypertension was driven by females (OR = 1.1, p-value = 0.002, OR = 1.01 p-value = 0.2 in males). OSA PGSs were also associated with body fat measures with some sex-specific associations.
Distinct components of OSA genetic risk are related and independent of obesity. Sex-specific associations with body fat distribution measures may explain differing OSA risks and associations with cardiometabolic morbidities between sexes.
R01AG080598.
阻塞性睡眠呼吸暂停(OSA)是一种常见的慢性疾病,肥胖是其最强的风险因素。多基因评分(PGS)总结了表型的遗传易感性,并能为表型之间的关系提供见解。最近,包含遗传数据和OSA状态的大型数据集变得可用,这为利用PGS方法研究OSA与其他表型之间的遗传关系提供了机会,同时区分OSA特异性和肥胖特异性遗传因素。
我们使用了来自百万退伍军人计划、芬兰基因研究、TOPMed、全民计划(AoU)、盖辛格的MyCode、MGB生物银行和人类表型项目的120多万名个体的种族/族裔多样化样本,开发并评估了OSA的PGS,一种未对体重指数(BMI)的遗传贡献进行调整(BMI未调整的OSA-PGS),另一种对BMI的遗传贡献进行了调整(BMI调整的OSA-PGS)。
PGS每增加1个标准差,OSA的调整后比值比(OR)范围为1.38至2.75。在AoU中,BMI调整的OSA-PGS和BMI未调整的OSA-PGS与心血管疾病结局的关联既有共同模式,也有不同模式。只有BMI未调整的OSA-PGS与2型糖尿病、心力衰竭和冠状动脉疾病相关,而BMI调整的OSA-PGS和BMI未调整的OSA-PGS均与高血压和中风相关。性别分层分析显示,BMI调整的OSA-PGS与高血压的关联在女性中更为明显(OR = 1.1,p值 = 0.002,男性中OR = 1.01,p值 = 0.2)。OSA PGS也与身体脂肪测量指标相关,且存在一些性别特异性关联。
OSA遗传风险的不同组成部分与肥胖相关且相互独立。与身体脂肪分布测量指标的性别特异性关联可能解释了男女之间OSA风险和与心血管代谢疾病关联的差异。
R01AG080598。