Shaban Eman, Khashaba Eman, Bassam Ensaf, Abdelaziz Ayman A, Shaban Amira, Shaban Ahmed, Zaki Hany A
Cardiology, Al Jufairi Diagnostic And Treatment, Doha, QAT.
Public Health and Community, Faculty of Medicine, Mansoura University, Mansoura, EGY.
Cureus. 2025 May 6;17(5):e83551. doi: 10.7759/cureus.83551. eCollection 2025 May.
This study aimed to assess the impact of socioeconomic status (SES) primarily on in-hospital outcomes, while also exploring its association with the incidence of acute myocardial infarction (AMI).
This was a case-control study that included 100 patients with first-onset AMI and 100 age- and sex-matched controls without clinical or investigative evidence of cardiac disease, confirmed by history, ECG, and absence of prior hospitalizations. Data collection involved demographics, cardiovascular risk factors (e.g., smoking, obesity, hypertension), blood pressure, BMI, echocardiography, and laboratory investigations, used diagnostically and prognostically. SES was assessed at admission using the Egyptian socioeconomic scale (total score: 84), covering seven domains. SES was categorized into very low (<40), low (40-56.9), middle (57-64.9), and high (>65). Assessing SES before outcome measurement reduced reverse causation risk.
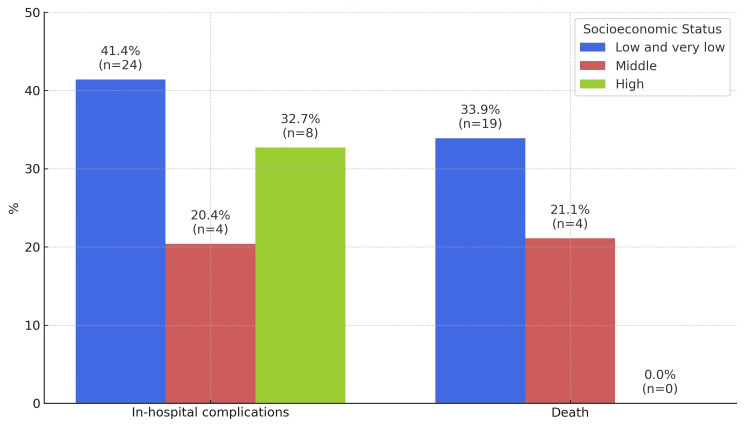
Occurrences and in-hospital outcomes, such as cardiogenic shock, were significantly more common among AMI patients from lower SES groups compared to higher SES groups (p < 0.05). Mortality was also higher in the lower SES group, with an odds ratio of 4.8 (95% confidence interval (CI): 1.5-16.6), indicating a more than fourfold increased risk. However, the wide CI suggests some uncertainty in the estimate, likely due to the limited sample size. In-hospital complications were reported in 41.1% of patients with low and very low SES (39 patients), compared to 20.4% (21 patients) and 32.7% (32 patients) in the middle and high SES groups, respectively.
These findings highlight that SES significantly shapes in-hospital outcomes among patients with first-onset AMI. Patients from lower SES groups experienced more frequent complications and higher mortality. While comorbid conditions such as hypertension, diabetes, and obesity were more prevalent in lower SES groups, SES itself served as the primary exposure variable influencing outcomes, rather than being evaluated through the presence of comorbidities.
本研究旨在评估社会经济地位(SES)主要对住院结局的影响,同时探讨其与急性心肌梗死(AMI)发病率的关联。
这是一项病例对照研究,纳入了100例首次发作AMI的患者以及100例年龄和性别匹配的无心脏病临床或检查证据的对照者,通过病史、心电图及无既往住院史进行确认。数据收集包括人口统计学、心血管危险因素(如吸烟、肥胖、高血压)、血压、BMI、超声心动图以及用于诊断和预后评估的实验室检查。入院时使用埃及社会经济量表(总分:84分)评估SES,该量表涵盖七个领域。SES分为极低(<40)、低(40 - 56.9)、中(57 - 64.9)和高(>65)。在结局测量前评估SES可降低反向因果关系风险。
与较高SES组相比,较低SES组的AMI患者发生心源性休克等住院结局的情况明显更为常见(p < 0.05)。较低SES组的死亡率也更高,比值比为4.8(95%置信区间(CI):1.5 - 16.6),表明风险增加了四倍多。然而,较宽的CI表明估计存在一定不确定性,可能是由于样本量有限。SES低和极低的患者中有41.1%(39例患者)报告了住院并发症,而SES中、高组分别为20.4%(21例患者)和32.7%(32例患者)。
这些发现突出表明,SES显著影响首次发作AMI患者的住院结局。较低SES组的患者并发症更频繁,死亡率更高。虽然高血压、糖尿病和肥胖等合并症在较低SES组中更为普遍,但SES本身是影响结局的主要暴露变量,而非通过合并症的存在来评估。