Kakamad Fahmi H, Hama Amin Bnar J, Salih Abdulwahid M, Mohammed Shvan H, Baba Hiwa O, Ahmed Gasha S, Tahir Soran H, Salih Rawezh Q, Abdalla Berun A, Hussein Dahat H, Kakamad Suhaib H, Hamasalih Hussein M, Mohammed Mohammed Subhan
College of Medicine, University of Sulaimani, Sulaymaniyah, Iraq.
Kscien Organization for Scientific Research (Middle East Office), Sulaymaniyah, Iraq.
Ann Med Surg (Lond). 2025 Apr 10;87(6):3215-3220. doi: 10.1097/MS9.0000000000003233. eCollection 2025 Jun.
This study explores whether using a separate incision for pleural drainage will yield superior results compared to inserting a chest drain through the utility incision in patients with operable lung cancer undergoing single utility port video-assisted thoracoscopic lobectomy.
Which one is the best?! Inserting the drain through the utility incision or separate incision in a single utility port video-assisted thoracoscopic lobectomy for lung cancer.
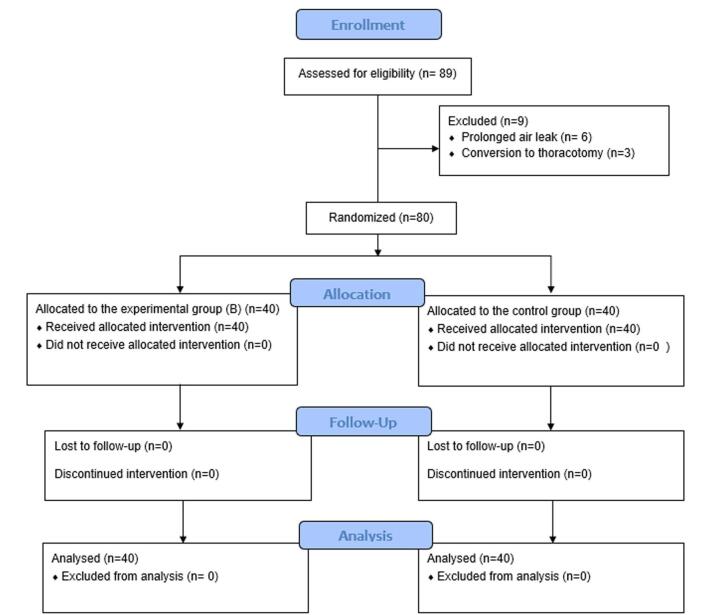
This was a randomized, open-label, superiority trial including patients with bronchogenic carcinoma who underwent a single utility port video-assisted thoracoscopic lobectomy over a 32-month period. The primary outcome was wound infections and postoperative pain, while the secondary outcomes were the duration of hospitalization and return to work.
The study included 89 patients, and 80 patients completed the trial. The mean age was 65.35 ± 9.47 years, 64 (80%) patients were male, and 69 (86.25%) patients had a 0 ECOG score. Eleven patients (13.75%) had a score of 1. The majority of the patients (35%) were in stage IIIA. There was a small but statistically significant difference in return to work when comparing group A with group B (34 ± 6 vs 31 ± 4 days, = 0.038). More important were the differences in patients with wound discharge (29 vs 4; < 0.001) and especially the need for intravenous antibiotic treatment (12 vs 1; < 0.002). There was only a minimal trend for a decrease in the duration of hospitalization. There was no significant difference in postoperative pain scores.
Inserting the chest drain through a separate incision has superior results compared to inserting it through the utility incision in patients with operable lung cancer undergoing single-port video-assisted thoracoscopic lobectomy. However, more studies with a larger sample size are necessary to confirm these results.
The research was registered in the Research Registry. The registration number is researchregistry8426. The link is https://www.researchregistry.com/register-now#home/?view_2_search=researchregistry8426&view_2_page=1.
本研究探讨在接受单操作孔电视辅助胸腔镜肺叶切除术的可手术肺癌患者中,与通过操作孔插入胸腔引流管相比,采用单独切口进行胸腔引流是否能产生更好的效果。
哪一种方法最佳?!在单操作孔电视辅助胸腔镜肺癌肺叶切除术中,通过操作孔插入引流管还是采用单独切口插入引流管。
这是一项随机、开放标签的优效性试验,纳入了在32个月期间接受单操作孔电视辅助胸腔镜肺叶切除术的支气管癌患者。主要结局是伤口感染和术后疼痛,次要结局是住院时间和恢复工作时间。
该研究纳入了89例患者,80例患者完成了试验。平均年龄为65.35±9.47岁,64例(80%)为男性,69例(86.25%)患者的东部肿瘤协作组(ECOG)评分为0分。11例(13.75%)患者评分为1分。大多数患者(35%)处于ⅢA期。比较A组和B组时,恢复工作时间存在微小但具有统计学意义的差异(34±6天对31±4天,P = 0.038)。更重要的是伤口渗液患者的差异(29例对4例,P<0.001),尤其是静脉使用抗生素治疗的需求差异(12例对1例,P<0.002)。住院时间仅有轻微的下降趋势。术后疼痛评分无显著差异。
在接受单操作孔电视辅助胸腔镜肺叶切除术的可手术肺癌患者中,与通过操作孔插入胸腔引流管相比,通过单独切口插入胸腔引流管具有更好的效果。然而,需要更多样本量更大的研究来证实这些结果。
该研究已在研究注册库注册。注册号为researchregistry8426。链接为https://www.researchregistry.com/register-now#home/?view_2_search=researchregistry8426&view_2_page=1。