Song Yongbin, Zheng Chong, Zhou Shaohui, Cui Hongshang, Wang Jincong, Wang Jianxun, Wang Wenhao, Liu Lijun, Liu Junfeng
Graduate School, Hebei Medical University, 361 Zhongshan East Road, Shijiazhuang, 050051, Hebei Province, People's Republic of China.
Department of Thoracic Surgery, Hebei General Hospital, 348 West He-Ping Road, Shijiazhuang, 050051, Hebei Province, People's Republic of China.
J Cardiothorac Surg. 2021 Apr 21;16(1):104. doi: 10.1186/s13019-021-01479-x.
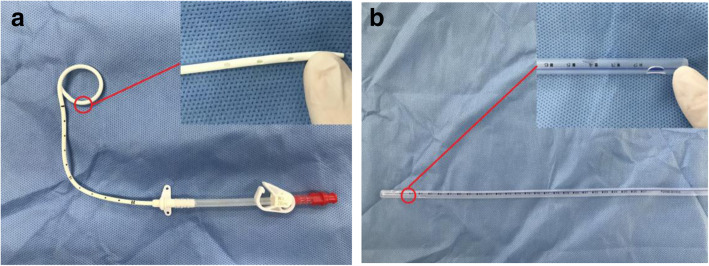
Currently, thoracoscopic lobectomy is widely used in clinical practice, and postoperative placement of ultrafine drainage tube has advantages of reducing postoperative pain and accelerating postoperative recovery in patients. This study aimed to investigate the feasibility and safety of placement of 8F ultrafine chest drainage tube after thoracoscopic lobectomy and its superiority over traditional 24F chest drainage tube.
A retrospective data analysis was conducted in 169 patients who underwent placement of 8F ultrafine chest drainage tube or 24F chest drainage tube with thoracoscopic lobectomy for lung cancer from January 2018 to December 2019. Propensity score matching (PSM) was used to reduce bias between the experimental group and the control group. After PSM, 134 patients (67 per group) were enrolled. The drainage time, the total drainage volume, postoperative hospital stay, postoperative pain score and postoperative complication of both groups were analyzed and compared.
Compared to group B, group A had lower pain scores on postoperative days 1, 2 and 3 (3.72 ± 0.65point vs 3.94 ± 0.67point, P = 0.027; 2.72 ± 0.93point vs 3.13 ± 1.04point, P = 0.016; and 1.87 ± 0.65point vs 2.39 ± 1.22point, P = 0.005), shorter drainage time (4.25 ± 1.79d vs 6.04 ± 1.96d, P = 0.000), fewer drainage volume (1100.42 ± 701.57 ml vs 1369.39 ± 624.25 ml, P = 0.021); and shorter postoperative hospital stay (8.46 ± 2.48d vs 9.37 ± 1.70d, P = 0.014). Postoperative complications such as subcutaneous emphysema, pulmonary infection, atelectasis, chest tube reinsertion and intrathoracic hemorrhage showed no differences between both groups (P > 0.05).
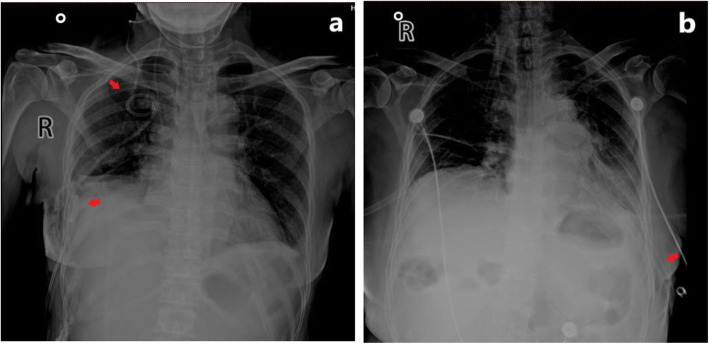
Compared with 24F chest drainage tube, the application of an 8F ultrafine chest drainage tube after thoracoscopic lobectomy has significantly shortened the drainage time, reduced the total drainage volume, reduced the postoperative pain degree, shortened the hospital day, and effectively detected postoperative intrathoracic hemorrhage. So, it is considered as an effective, safe and reliable drainage method.
目前,胸腔镜肺叶切除术在临床实践中广泛应用,术后放置超细引流管具有减轻患者术后疼痛和加速术后恢复的优点。本研究旨在探讨胸腔镜肺叶切除术后放置8F超细胸腔引流管的可行性和安全性及其优于传统24F胸腔引流管的地方。
对2018年1月至2019年12月期间因肺癌接受胸腔镜肺叶切除术并放置8F超细胸腔引流管或24F胸腔引流管的169例患者进行回顾性数据分析。采用倾向评分匹配(PSM)以减少实验组和对照组之间的偏差。PSM后,纳入134例患者(每组67例)。分析并比较两组的引流时间、总引流量、术后住院时间、术后疼痛评分和术后并发症。
与B组相比,A组在术后第1、2和3天的疼痛评分更低(3.72±0.65分 vs 3.94±0.67分,P = 0.027;2.72±0.93分 vs 3.13±1.04分,P = 0.016;1.87±0.65分 vs 2.39±1.22分,P = 0.005),引流时间更短(4.25±1.79天 vs 6.04±1.96天,P = 0.000),引流量更少(1100.42±701.57 ml vs 1369.39±624.25 ml,P = 0.021);术后住院时间更短(8.46±2.48天 vs 9.37±1.70天,P = 0.014)。两组术后并发症如皮下气肿、肺部感染、肺不张、胸腔闭式引流管重置和胸腔内出血无差异(P>0.05)。
与24F胸腔引流管相比,胸腔镜肺叶切除术后应用8F超细胸腔引流管显著缩短了引流时间,减少了总引流量,减轻了术后疼痛程度,缩短了住院天数,并能有效检测术后胸腔内出血。因此,它被认为是一种有效、安全且可靠的引流方法。