Mittman Benjamin G, Rothberg Michael B
Medical Scientist Training Program, School of Medicine, Case Western Reserve University, Cleveland, OH, USA.
Center for Value-Based Care Research, Primary Care Institute, Cleveland Clinic, Cleveland, OH, USA.
medRxiv. 2025 May 31:2025.05.29.25328593. doi: 10.1101/2025.05.29.25328593.
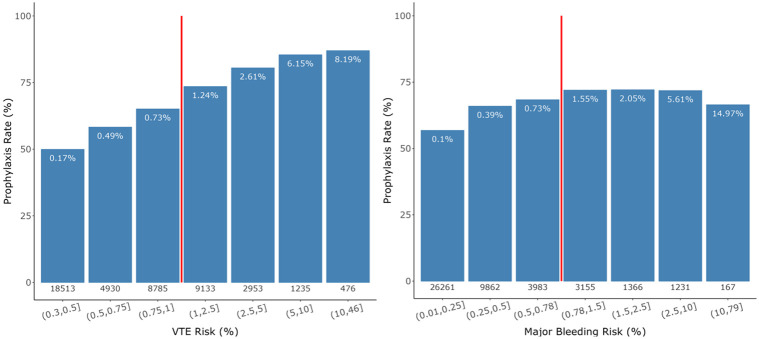
The American Society of Hematology (ASH) recommends assessing venous thromboembolism (VTE) and major bleeding risk to optimize pharmacological VTE prophylaxis for medical inpatients. However, the clinical utility of model-guided approaches remains unknown.
Our objective was to estimate differences in VTE and major bleeding event rates and efficiency with prophylaxis guided by risk models versus prophylaxis based on physician judgment. Patients were adults admitted to one of 10 Cleveland Clinic hospitals between December 2017 and January 2020. We compared physician practice with hypothetical prophylaxis recommended by model-based prophylaxis strategies, including ASH-recommended risk scores (Padua and IMPROVE) and locally derived Cleveland Clinic risk prediction models. For each strategy we quantified the prophylaxis rate, VTE and major bleeding rates, and the incremental number-needed-to-treat (NNT) to prevent one event (VTE or bleeding).
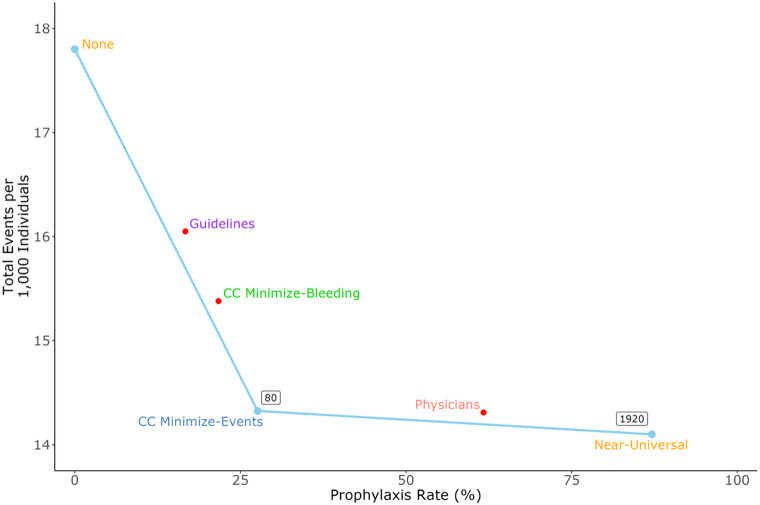
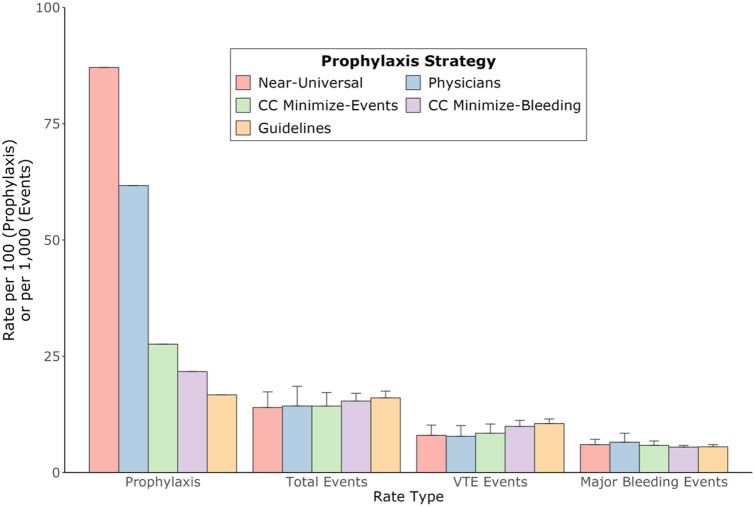
Physicians prescribed prophylaxis to 62% of patients whereas model-based strategies recommended prophylaxis for 17-87%. Model-guided prophylaxis produced more VTEs and fewer major bleeds than physicians, but total events varied among strategies. Overall, per 1,000 patients, model-based strategies produced 14.0-16.1 events compared with 14.3 for physicians. The Padua/IMPROVE models recommended prophylaxis for the fewest patients but caused the most total events. The most efficient model-based strategy recommended prophylaxis to 28% of patients with an incremental NNT (relative to no prophylaxis) of 80. Compared to physicians, it reduced prophylaxis by 55% and total events by 0.14%.
Physicians often prescribed inappropriate prophylaxis, highlighting the need for decision support. A model-based strategy maximized efficiency, reducing both events and prophylaxis relative to physicians.
美国血液学会(ASH)建议评估静脉血栓栓塞(VTE)和大出血风险,以优化对内科住院患者的药物性VTE预防。然而,模型指导方法的临床实用性仍不明确。
我们的目标是估计风险模型指导下的预防与基于医生判断的预防在VTE和大出血事件发生率及效率方面的差异。患者为2017年12月至2020年1月期间入住克利夫兰诊所10家医院之一的成年人。我们将医生的做法与基于模型的预防策略推荐的假设性预防措施进行了比较,包括ASH推荐的风险评分(帕多瓦和IMPROVE)以及克利夫兰诊所本地得出的风险预测模型。对于每种策略,我们量化了预防率、VTE和大出血率,以及预防一例事件(VTE或出血)所需的增量治疗人数(NNT)。
医生为62%的患者开具了预防措施,而基于模型的策略推荐预防的比例为17%-87%。模型指导的预防措施比医生导致更多的VTE和更少的大出血,但不同策略的总事件数有所不同。总体而言,每1000名患者中,基于模型的策略产生14.0-16.1起事件,而医生为14.3起。帕多瓦/IMPROVE模型推荐预防的患者最少,但导致的总事件数最多。最有效的基于模型的策略为28%的患者推荐预防措施,增量NNT(相对于不预防)为80。与医生相比,它将预防措施减少了55%,总事件数减少了0.14%。
医生经常开具不适当的预防措施,凸显了决策支持的必要性。基于模型的策略使效率最大化,相对于医生而言,减少了事件和预防措施。