Garne Ester, Damkjær Mads, Rissmann Anke, Cavero-Carbonell Clara, Gissler Mika, Neville Amanda, Santoro Michele, Tan Joachim, Tucker David, Loane Maria, Morris Joan
Department of Paediatrics and Adolescent Medicine, Lillebaelt Hospital, University Hospital of Southern Denmark, Sygehusvej 24, 6000, Kolding, Denmark.
Medical Faculty, Malformation Monitoring Centre Saxony-Anhalt, Otto-Von-Guericke-University Magdeburg, Magdeburg, Germany.
Eur J Pediatr. 2025 Jun 10;184(7):414. doi: 10.1007/s00431-025-06232-3.
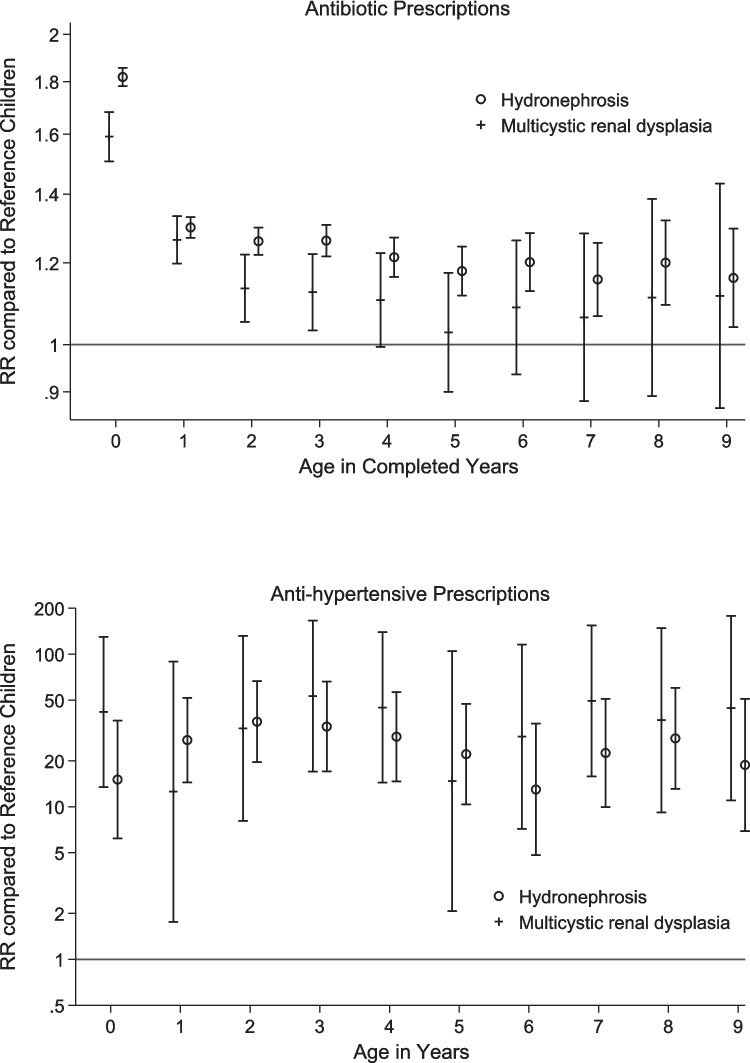
Knowledge about the prognosis for children born with congenital anomalies is important for counselling parents after a prenatal diagnosis. Nine population-based European Congenital Anomaly registries provided data on all children born 1995-2014 diagnosed with congenital hydronephrosis, multicystic kidney disease (MCKD), or posterior urethral valves (PUV) and on reference children from the same populations. Data up to 2015 on prescriptions, hospital diagnosis, and surgical procedures up to the 10th birthday were obtained by linkage to prescription and hospital databases. The study included 5624 children diagnosed with congenital hydronephrosis, 1314 with MCKD, and 414 with PUV. Children with hydronephrosis or MCKD were 13 times more likely to have prescriptions for antihypertensives compared to reference children before 10 years of age. Around 3% of children with congenital hydronephrosis or MCKD had a diagnosis of kidney failure at the age of 5 years; however, only 1% had a kidney transplantation by the age of 5 years. For children with PUV, 18.3% had a diagnosis of kidney failure and 5% had a kidney transplantation by the age of 5 years.
Children born with congenital hydronephrosis and MCKD generally have a low absolute risk of developing kidney failure. Children with PUV have much higher morbidity, with 1 in 5 (18.3%) being diagnosed with kidney failure before the age of 5 years. It is important to monitor these children closely in early childhood in order to prevent or delay kidney failure.
• Congenital kidney anomalies are a leading cause of pediatric end-stage kidney disease. Children with hydronephrosis, MCKD, and PUV have increased morbidity, but long-term data on medication use and kidney outcomes are limited.
• This population-based study shows a low absolute risk of kidney failure in children born with hydronephrosis or MCKD but a high relative risk. PUV has high morbidity, with 1 in 4 developing kidney failure by age 10. Antibiotic use is high in early childhood, and antihypertensive use increases with age.
了解先天性异常患儿的预后情况对于产前诊断后向家长提供咨询很重要。九个基于人群的欧洲先天性异常登记处提供了1995年至2014年出生的所有被诊断为先天性肾积水、多囊肾病(MCKD)或后尿道瓣膜(PUV)的儿童以及来自相同人群的对照儿童的数据。通过与处方和医院数据库进行关联,获取了截至2015年这些儿童在10岁生日前的处方、医院诊断和手术程序数据。该研究纳入了5624例被诊断为先天性肾积水的儿童、1314例MCKD患儿和414例PUV患儿。10岁前,肾积水或MCKD患儿开具抗高血压药处方的可能性是对照儿童的13倍。约3%的先天性肾积水或MCKD患儿在5岁时被诊断为肾衰竭;然而,5岁时只有1%的患儿接受了肾移植。对于PUV患儿,18.3%在5岁时被诊断为肾衰竭,5%在5岁时接受了肾移植。
先天性肾积水和MCKD患儿发生肾衰竭的绝对风险通常较低。PUV患儿的发病率要高得多,五分之一(18.3%)的患儿在5岁前被诊断为肾衰竭。在儿童早期密切监测这些患儿以预防或延缓肾衰竭很重要。
•先天性肾脏异常是儿童终末期肾病的主要原因。肾积水、MCKD和PUV患儿的发病率增加,但关于药物使用和肾脏结局的长期数据有限。
•这项基于人群的研究表明,先天性肾积水或MCKD患儿发生肾衰竭的绝对风险较低,但相对风险较高。PUV发病率高,四分之一的患儿在10岁时发生肾衰竭。儿童早期抗生素使用频繁,抗高血压药的使用随年龄增加。