Lugata John, Makower Laetitia, Hita Bariza, Lyamuya Tecla
Department of Obstetrics and Gynecology, Kilimanjaro Christian Medical Centre, Moshi, Tanzania; Faculty of Medicine, Kilimanjaro Christian Medical University College, Moshi, Tanzania.
School of Clinical Medicine, University of Cambridge, Cambridge, United Kingdom.
Int J Surg Case Rep. 2025 Jul;132:111484. doi: 10.1016/j.ijscr.2025.111484. Epub 2025 Jun 7.
Intestinal obstruction is a rare but serious condition in pregnancy, posing significant risks to both maternal and fetal health. Its diagnosis and management are particularly challenging due to non-specific symptoms, limitations in radiological assessment during pregnancy, and the potential for surgical complications. The differentiation between obstetric and non-obstetric causes of an acute abdomen also poses a diagnostic challenge. To the best of our knowledge, this study reports one of the rarest cases of intestinal obstruction in the first trimester of pregnancy. The case was initially mistaken for an ectopic pregnancy. The condition was successfully managed surgically without the need for pregnancy termination.
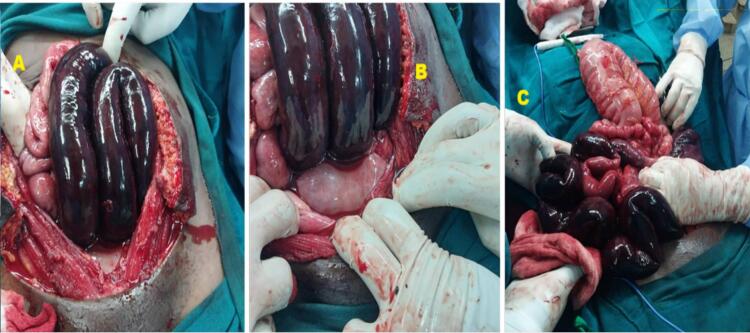
A 34-year-old G3P2L2 woman from Northern Tanzania presented at 12 weeks gestation with sudden-onset abdominal pain. Initial radiological findings suggested a ruptured ectopic pregnancy with extensive hemoperitoneum. The patient was taken for an emergency laparotomy where an intrauterine pregnancy was identified as well as gangrenous small bowel and sigmoid colon due to a 360-degree mesenteric rotation. Surgical intervention included bowel resection, decompression, and anastomosis of the remaining segments. The mesenteric defects were closed, and the patient had an uneventful postoperative recovery, being discharged in stable condition for conservative management.
This case report highlights the rarity of intestinal obstruction during pregnancy and the diagnostic challenges it presents. Our case is particularly unique due to the absence of previous abdominal surgery and presentation so early in gestation. There exists significant diagnostic uncertainty and resulting delays in treatment have the potential to increase the risk of maternal and fetal morbidity, especially in resource poor settings.
Intestinal obstruction during pregnancy is an uncommon but serious condition associated with significant maternal and fetal morbidity. Its diagnosis can be challenging, as symptoms may mimic common obstetric complications, leading to potential delays in recognition and treatment. Effective management requires a multidisciplinary approach and timely clinical decision-making to optimize outcomes for both the mother and fetus.
肠梗阻在妊娠中是一种罕见但严重的病症,对母婴健康均构成重大风险。由于症状不具特异性、孕期放射学评估存在局限性以及手术并发症的可能性,其诊断和管理极具挑战性。区分急腹症的产科和非产科病因也带来了诊断难题。据我们所知,本研究报告了妊娠早期最罕见的肠梗阻病例之一。该病例最初被误诊为异位妊娠。该病症通过手术成功治疗,无需终止妊娠。
一名来自坦桑尼亚北部的34岁经产妇(孕3产2,足月产2次),妊娠12周时出现突发腹痛。最初的放射学检查结果提示异位妊娠破裂伴大量腹腔积血。患者接受了急诊剖腹探查术,术中发现宫内妊娠,同时还发现因肠系膜360度旋转导致的坏疽性小肠和乙状结肠。手术干预包括肠切除、减压以及剩余肠段的吻合。肠系膜缺损得以闭合,患者术后恢复顺利,出院时情况稳定,接受保守治疗。
本病例报告突出了妊娠期间肠梗阻的罕见性及其带来的诊断挑战。我们的病例尤为独特,因为患者既往无腹部手术史且妊娠早期即出现症状。存在显著的诊断不确定性,由此导致的治疗延误有可能增加母婴发病风险,尤其是在资源匮乏地区。
妊娠期间的肠梗阻是一种不常见但严重的病症,与母婴显著发病相关。其诊断可能具有挑战性,因为症状可能类似常见的产科并发症,导致识别和治疗可能延误。有效的管理需要多学科方法和及时的临床决策,以优化母婴结局。