Süer Onur, Ozturk Anıl Murat, Tamsel Ipek, Aktuglu Kemal
Department of Orthopaedics and Traumatology, Izmir City Hospital, İzmir-Türkiye.
Department of Orthopaedics Surgery, Ege University Faculty of Medicine, İzmir-Türkiye.
Ulus Travma Acil Cerrahi Derg. 2025 Jun;31(6):577-586. doi: 10.14744/tjtes.2025.69886.
Rotational malalignment following intramedullary nailing (IMN) of femoral shaft fractures remains a clinically significant concern, with previous studies reporting variable incidence rates and inconsistent risk factors. This study aimed to determine the incidence of rotational malalignment after closed static-locked intramedullary nailing for adult diaphyseal femoral fractures, identify contributing etiological factors, and evaluate its clinical impact on functional capacity and quality-of-life metrics.
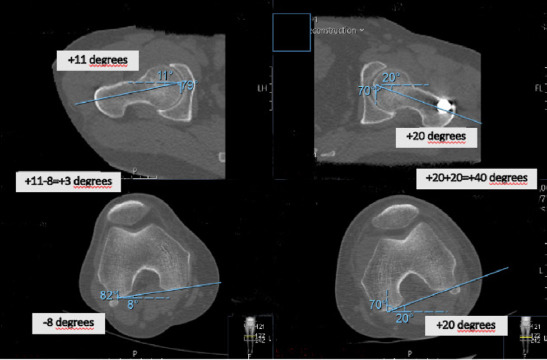
A retrospective cohort study was conducted involving 54 adults treated with closed static-locked IMN for diaphyseal femur fractures between 2014 and 2019. Rotational alignment was assessed using computed tomography (CT)-measured femoral anteversion (FAV) differences, with a threshold of ≥15° defined as malalignment. Multivariate logistic regression was employed to examine associations with fracture pattern, nail entry site, surgical timing (day vs. night), and coronal alignment. Functional outcomes were assessed using the WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index) knee, Harris hip, Lower Extremity Functional Scale, and Kujala patellofemoral scores. Receiver operating characteristic (ROC) analysis was used to determine optimal FAV thresholds.
Rotational malalignment (≥15° FAV difference) was observed in 33.3% of cases, with 94.4% involving internal rotation. Multivariate analysis identified no independent predictors among the following factors: fracture location (proximal 44.4% vs. middle 29.2%, p=0.625), AO classification (Type A 34.3% vs. Type C 33.3%, p=0.914), nail entry site (lateral trochanteric 40% vs. piriformis 16.6%, p=0.574), and surgical timing (night 26.1% vs. day 38.7%, p=0.228). Patients with malalignment demonstrated significantly poorer functional outcomes, as evidenced by higher WOMAC knee scores (12.7+-4.8 vs. 6.4+-4.8, p<0.001). ROC curve analysis identified 13.5° as the optimal FAV threshold (area under the curve, AUC: 0.78), although the 15° cutoff maintained strong clinical utility with a specificity of 83%.
Rotational malalignment following IMN occurs in one-third of cases and has a significant negative impact on functional outcomes. However, it appears to be independent of commonly considered surgical variables such as entry site and timing. These findings support technical flexibility in IMN procedures while highlighting the need for improved intraoperative techniques to assess rotational alignment.
股骨干骨折髓内钉固定术后的旋转畸形仍然是临床上的一个重要问题,以往研究报告的发生率各不相同,危险因素也不一致。本研究旨在确定成人股骨干骨折闭合静态锁定髓内钉固定术后旋转畸形的发生率,确定相关病因,并评估其对功能能力和生活质量指标的临床影响。
进行一项回顾性队列研究,纳入2014年至2019年间54例接受闭合静态锁定髓内钉治疗股骨干骨折的成人患者。使用计算机断层扫描(CT)测量的股骨前倾角(FAV)差异评估旋转对线情况,≥15°的阈值定义为对线不良。采用多因素逻辑回归分析骨折类型、进钉点、手术时间(白天与夜间)和冠状面排列的相关性。使用WOMAC(西安大略和麦克马斯特大学骨关节炎指数)膝关节、Harris髋关节、下肢功能量表和Kujala髌股关节评分评估功能结果。采用受试者工作特征(ROC)分析确定最佳FAV阈值。
33.3%的病例观察到旋转畸形(FAV差异≥15°),94.4%为内旋。多因素分析未发现以下因素中有独立预测因素:骨折部位(近端44.