Laterza Vito, Covino Marcello, Schena Carlo Alberto, Della Polla Davide, Russo Andrea, Salini Sara, de'Angelis Nicola, Quero Giuseppe, Recupero Carla, Fiorillo Claudio, Risoli Antonella, Cina Caterina, Franceschi Francesco, Alfieri Sergio, Rosa Fausto
Department of Digestive Surgical Oncology and Liver Transplantation, University Hospital of Besançon, Besançon, France.
Università Cattolica del Sacro Cuore, Rome, Italy.
Int J Colorectal Dis. 2025 Jun 16;40(1):141. doi: 10.1007/s00384-025-04933-7.
Acute left-sided colonic diverticulitis (ALCD) has a more complicated course in older patients. Rather than age, frailty may be crucial in ALCD prognosis in this heterogeneous population. This study aims to define the influence of the Clinical Frailty Scale (CFS) on mortality and clinical outcomes in patients aged 70 or older with ALCD.
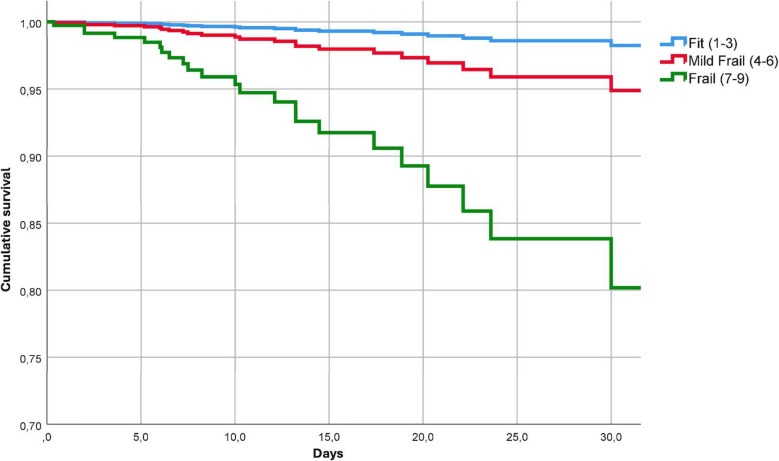
All patients aged ≥ 70 years admitted to the emergency department for ALCD between January 2018 and December 2022 were included. Frailty was assessed through the CFS, and three groups of patients were identified accordingly: non-frail patients (CFS 1-3); moderately frail patients (CFS 4-6); and severely frail patients (CFS 7-9). The endpoints were: 30-day mortality, sepsis onset, 30-day readmission, and length of hospital stay (LOS).
A total of 1127 patients were enrolled. Severely frail patients had a significantly higher rate of sepsis onset, mortality, and longer LOS at univariate analysis. Higher CFS scores were significantly associated with mortality, both as a continuous (OR 1.42) and discrete variable (OR 12.47), and sepsis, both as a continuous (OR 1.5) and discrete variable (OR 6.52) at multivariate analysis.
A higher CFS score, rather than age, is associated with higher rates of mortality, sepsis, and longer LOS. After adjusting for covariates, higher CFS scores were significantly associated with increased risk of 30-day mortality and sepsis. A comprehensive frailty assessment using the CFS should be considered to predict the need for closer monitoring and guiding appropriate care goals for older patients.
急性左侧结肠憩室炎(ALCD)在老年患者中病程更为复杂。在这个异质性群体中,衰弱而非年龄可能对ALCD的预后至关重要。本研究旨在确定临床衰弱量表(CFS)对70岁及以上ALCD患者死亡率和临床结局的影响。
纳入2018年1月至2022年12月期间因ALCD入住急诊科的所有年龄≥70岁的患者。通过CFS评估衰弱情况,并据此将患者分为三组:非衰弱患者(CFS 1-3);中度衰弱患者(CFS 4-6);重度衰弱患者(CFS 7-9)。观察终点为:30天死亡率、脓毒症发作、30天再入院率和住院时间(LOS)。
共纳入1127例患者。在单因素分析中,重度衰弱患者的脓毒症发作率、死亡率显著更高,住院时间更长。在多因素分析中,较高的CFS评分与死亡率显著相关,无论是作为连续变量(OR 1.42)还是离散变量(OR 12.47),与脓毒症也显著相关,无论是作为连续变量(OR 1.5)还是离散变量(OR 6.52)。
较高的CFS评分而非年龄与更高的死亡率、脓毒症发生率和更长的住院时间相关。在调整协变量后,较高的CFS评分与30天死亡率和脓毒症风险增加显著相关。应考虑使用CFS进行全面的衰弱评估,以预测老年患者密切监测的需求并指导适当的护理目标。