Giordano Giulia, Mastrantoni Luca, Landi Francesco
Department of Geriatrics, Orthopedics and Rheumatological Sciences, Fondazione Policlinico Universitario Agostino Gemelli, IRCCS, Rome, Italy.
Department of Geriatrics, Orthopedics and Rheumatological Sciences, Università Cattolica del Sacro Cuore, Rome, Italy.
J Cachexia Sarcopenia Muscle. 2025 Jun;16(3):e13868. doi: 10.1002/jcsm.13868.
Muscle strength is one of the key components in the diagnosis of sarcopenia. The aim of this study was to train a machine learning model to predict reference values and percentiles for handgrip strength and chair-stand test (CST), in a large cohort of community dwellers recruited in the Longevity check-up (Lookup) 8+ project.
The longevity checkup project is an ongoing initiative conducted in unconventional settings in Italy from 1 June 2015. Eligible participants were 18+ years and provided written informed consent. After a 70/20/10 split in training, validation and test set, a quantile regression forest (QRF) was trained. Performance metrics were R-squared (R), mean squared error (MSE), root mean squared error (RMSE) and mean Winkler interval score (MWIS) with 90% prediction coverage (PC). Metrics 95% confidence intervals (CI) were calculated using a bootstrap approach. Variable contribution was analysed using SHapley Additive exPlanations (SHAP) values. Probable sarcopenia (PS) was defined according to the European Working Group on Sarcopenia in Older People 2 (EWGSOP2) criteria.
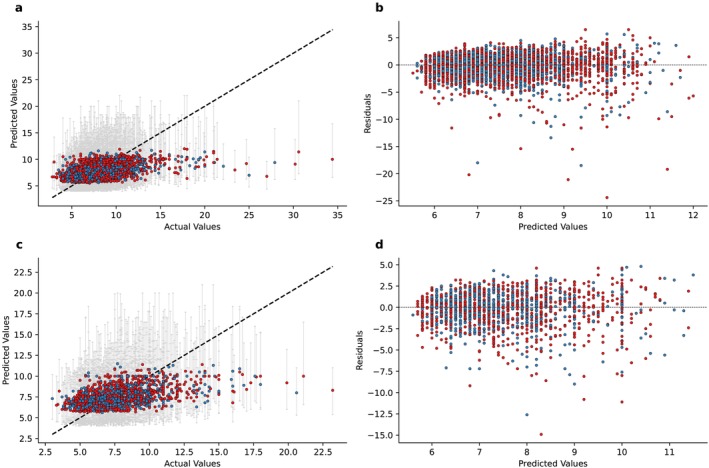
Between 1 June 2015 and 23 November 2024, a total of 21 171 individuals were enrolled, of which 19 995 were included in our analyses. In the overall population, 11 019 (55.1%) were females. Median age was 56 years (IQR 47.0-67.0). Five variables were included: age, sex, height, weight and BMI. After the train/validation/test split, 13 996 subjects were included in the train set, 4199 in validation set and 1800 in the test set. For handgrip strength, the R was 0.65 (95% CI 0.63-0.67) in the validation set and 0.64 (95% CI 0.62-0.67) in the test set. PCs were 91.5% and 91.2%, respectively. For CST test, the R was 0.23 (95% CI 0.20-0.25) in the validation set and 0.24 (95% CI 0.20-0.28) in the test set. The PCs were 89.5% and 89.3%. Gender was the most influential variable for handgrip and age for CST. In the validation set, 23% of subjects in the first quartile for handgrip and 13% of subjects in the fourth quartile for CST test met criteria of PS.
We developed and validated a QRF model to predict subject-specific quantiles for handgrip and CST. These models hold promise for integration into clinical practice, facilitating cost-effective and time-efficient early identification of individuals at elevated risk of sarcopenia. The predictive outputs of these models may serve as surrogate biomarkers of the aging process, capturing functional decline.
肌肉力量是肌少症诊断的关键组成部分之一。本研究的目的是训练一个机器学习模型,以预测长寿体检(Lookup)8 +项目招募的大量社区居民的握力和椅子起立测试(CST)的参考值和百分位数。
长寿体检项目是一项于2015年6月1日起在意大利非传统环境中开展的正在进行的倡议。符合条件的参与者年龄在18岁及以上,并提供了书面知情同意书。在按70/20/10比例划分训练集、验证集和测试集后,训练了一个分位数回归森林(QRF)。性能指标包括决定系数(R)、均方误差(MSE)、均方根误差(RMSE)和具有90%预测覆盖率(PC)的平均温克勒区间得分(MWIS)。使用自助法计算指标的95%置信区间(CI)。使用夏普利值(SHAP)分析变量贡献。根据欧洲老年人肌少症工作组2(EWGSOP2)标准定义可能的肌少症(PS)。
在2015年6月1日至2024年11月23日期间,共招募了21171人,其中19995人纳入我们的分析。在总体人群中,11019人(55.1%)为女性。年龄中位数为56岁(四分位间距47.0 - 67.0)。纳入了五个变量:年龄、性别、身高、体重和体重指数。在进行训练/验证/测试划分后,训练集中有13996名受试者,验证集中有4199名受试者,测试集中有1800名受试者。对于握力,验证集中的R为0.65(95%CI 0.63 - 0.67),测试集中为0.64(95%CI 0.62 - 0.67)。预测覆盖率分别为91.5%和91.2%。对于CST测试,验证集中的R为0.23(95%CI 0.20 - 0.25),测试集中为0.24(95%CI 0.20 - 0.28)。预测覆盖率分别为89.5%和89.3%。性别是握力最具影响力的变量,年龄是CST测试最具影响力的变量。在验证集中,握力处于第一四分位数的受试者中有23%,CST测试处于第四四分位数的受试者中有13%符合PS标准。
我们开发并验证了一个QRF模型,以预测握力和CST的受试者特定分位数。这些模型有望整合到临床实践中,有助于经济高效且及时地早期识别肌少症风险升高的个体。这些模型的预测输出可作为衰老过程的替代生物标志物,反映功能衰退。