Nguyen Ha Thi Thu, Duong Giang Thi Tra, Do Dat Tuan, Phan Thuong Thi Huyen, Tran Duc Anh, Nguyen Toan Khac, Nguyen Anh Duy
National Center for Assisted Reproduction, National Hospital of Obstetrics and Gynecology, Hanoi, Vietnam (H. Nguyen).
Department of Obstetrics and Gynecology, Vietnam National University - University of Medicine and Pharmacy, Hanoi Vietnam (H. Nguyen).
AJOG Glob Rep. 2025 Jun 4;5(2):100507. doi: 10.1016/j.xagr.2025.100507. eCollection 2025 May.
There is an ongoing controversy regarding the optimal uterine closure technique for preventing niche development. Single- and double-layer closures have been considered comparable in terms of niche incidence after primary cesarean delivery. However, rather than simply the presence of a niche, its volume and residual myometrial thickness are the most potent factors in predicting gynecologic symptoms and subsequent pregnancy complications in women with cesarean scar defects. In addition, there is limited evidence on how uterine scars and niche sizes evolve over time.
This study aimed to compare the residual myometrial thickness and niche characteristics between the single-layer and double-layer uterine closure techniques and to evaluate the change in uterine scar characteristics from 6 to 12 months after cesarean delivery.
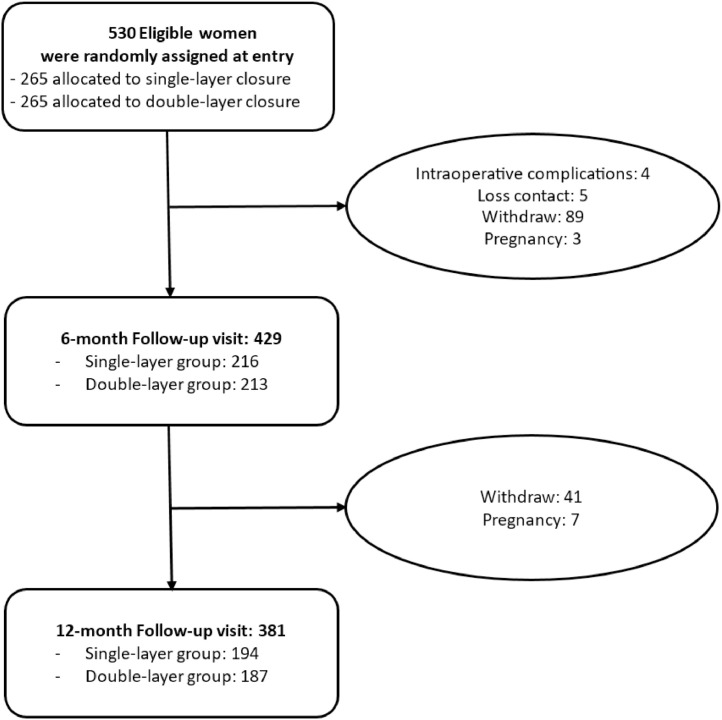
This prospective randomized study was conducted from May 2022 to December 2024 at Hanoi Obstetrics and Gynecology Hospital. A total of 530 full-term pregnant women who underwent primary cesarean delivery were randomized into single- or double-layer, unlocked, continuous suture. The exclusion criteria included previous major uterine surgery and abnormal placenta (placenta previa or placenta accreta spectrum) in the current pregnancy. Women were invited for 2 consecutive follow-up visits within 10 days of menstruation at 6 months (n=429) and 12 months (n=381) after cesarean delivery. Transvaginal ultrasound was used to evaluate uterine ultrasound characteristics. If the niche was detected, 3-dimensional transvaginal ultrasound was applied to measure the niche volume via the Virtual Organ Computer-aided AnaLysis method. Complete-case analysis was performed to evaluate the change in uterine ultrasound characteristics between the 2 visits.
Of 429 women who participated in the 6-month visit, 216 had single-layer closure, and 213 had double-layer closure. The niche incidence at the first assessment was similar for both uterine closure techniques, at 35.6% in the single-layer group and 31.9% in the double-layer group, respectively (>.05). At 6 months after delivery, the double-layer technique resulted in greater residual myometrial thickness (4.3 vs 4.0 mm; =.007), better healing ratio (69% vs 60%; =.048), and a lower proportion of large niches with residual myometrial thickness of <3 mm (9.9% vs 19.4%; =.033). The median niche volume in the single-layer group (62 mm) at 6 months after delivery was significantly higher than that in the double-layer group (39 mm) (=.003). Of 381 women who completed both assessments, 194 had single-layer closure, and 187 had double-layer closure. The results between the single-layer and double-layer groups of the second visit at 12 months after delivery mirrored those at the first visit. In longitudinal follow-up evaluation, uterine scar characteristics were stable, and the overall proportion of niches remained consistent from 6 months to 12 months after delivery, at 34.4% and 36.0%, respectively (>.05). There was an increase in niche length (5.0 vs 5.5 mm; =.000) and niche volume (47 vs 55 mm; =.000) among the assessments.
Although the niche incidence was similar between the 2 uterine closure techniques, the double-layer technique showed superior benefits, with greater residual myometrial thickness and healing ratio, lower large niche proportion, and smaller niche volume. The uterine scar characteristics were stable at 6 months after cesarean delivery, but the niche volume significantly increased over time. Future long-term follow-up research is needed to elucidate the relationship between niche size and clinical symptoms and to investigate the factors contributing to the temporal evolution of niche volume.
关于预防切口憩室形成的最佳子宫缝合技术一直存在争议。在初次剖宫产术后,单层和双层缝合在切口憩室发生率方面被认为相当。然而,对于剖宫产瘢痕缺损的女性,预测妇科症状和后续妊娠并发症的最有力因素不仅仅是切口憩室的存在,还包括其体积和剩余肌层厚度。此外,关于子宫瘢痕和切口憩室大小如何随时间演变的证据有限。
本研究旨在比较单层和双层子宫缝合技术之间的剩余肌层厚度和切口憩室特征,并评估剖宫产术后6至12个月子宫瘢痕特征的变化。
本前瞻性随机研究于2022年5月至2024年12月在河内妇产科医院进行。共有530例接受初次剖宫产的足月孕妇被随机分为单层或双层、非锁定连续缝合组。排除标准包括既往子宫大手术史和本次妊娠中的异常胎盘(前置胎盘或胎盘植入谱系)。邀请女性在剖宫产术后6个月(n = 429)和12个月(n = 381)月经来潮的10天内连续进行2次随访。经阴道超声用于评估子宫超声特征。如果检测到切口憩室,则应用三维经阴道超声通过虚拟器官计算机辅助分析方法测量切口憩室体积。进行完全病例分析以评估两次随访之间子宫超声特征的变化。
在参与6个月随访的429名女性中,216例行单层缝合,213例行双层缝合。两种子宫缝合技术在首次评估时的切口憩室发生率相似,单层组为35.6%,双层组为31.9%(P >.05)。产后6个月时,双层技术导致更大的剩余肌层厚度(4.3对4.0mm;P =.007)、更高的愈合率(69%对60%;P =.048)以及剩余肌层厚度<3mm的大切口憩室比例更低(9.9%对19.4%;P =.033)。产后6个月时,单层组的切口憩室中位体积(62mm)显著高于双层组(39mm)(P =.003)。在完成两次评估的381名女性中,194例行单层缝合,187例行双层缝合。产后12个月第二次随访时单层和双层组的结果与第一次随访相似。在纵向随访评估中,子宫瘢痕特征稳定,产后6个月至12个月切口憩室的总体比例保持一致,分别为34.4%和36.0%(P >.05)。两次评估之间切口憩室长度(5.0对5.5mm;P =.000)和切口憩室体积(47对55mm;P =.000)均增加。
尽管两种子宫缝合技术的切口憩室发生率相似,但双层技术显示出更好的效果,具有更大的剩余肌层厚度和愈合率、更低的大切口憩室比例以及更小的切口憩室体积。剖宫产术后6个月子宫瘢痕特征稳定,但切口憩室体积随时间显著增加。未来需要进行长期随访研究,以阐明切口憩室大小与临床症状之间的关系,并研究导致切口憩室体积随时间演变的因素。