Alexander S E, Mitchell R A, Dunlop A, Herbert T, Morrison K, Nartey J, Oelfke U, McNair H A, Tree A C
The Royal Marsden NHS Foundation Trust and the Institute of Cancer Research, UK.
The Joint Department of physics, the Royal Marsden Hospital and the Institute of Cancer Research, UK.
Clin Transl Radiat Oncol. 2025 Jun 3;53:100985. doi: 10.1016/j.ctro.2025.100985. eCollection 2025 Jul.
Magnetic resonance image-guided adaptive radiotherapy (MRIgART) reduces uncertainties by correcting for day-to-day target and organ-at-risk deformation and motion. This is the first study to examine the dosimetric impact of MRIgART for ultrahypofractionated prostate cancer treatment, compared to standard-of-care image-guided non-adapted radiotherapy.
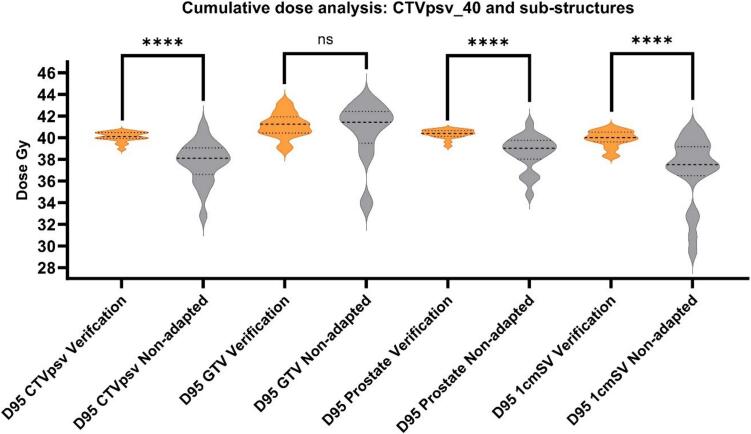
Twenty patients with localised prostate cancer, who received ultrahypofractionated MRIgART on the Unity MR linac (Elekta, Sweden) were retrospectively analysed. Online daily MRI was acquired for replanning (MRI) and a second for position verification before treatment (MRI). To compare delivered dose with and without adaptation, three plans were generated offline per fraction; a session plan (reference plan adapted to MRI anatomy), a verification plan (session plan recalculated on MRI anatomy), and a non-adapted plan (reference plan recalculated on MRI anatomy). Target and organ-at-risk doses were calculated, and dose difference evaluated.Secondary analysis, using deformable dose accumulation, estimated verification and non-adapted dose to primary target (CTVpsv) substructures; prostate, gross tumour volume (GTV) and proximal 1 cm of seminal vesicles (1cmSV). Impact of prostate, rectum and bladder volume changes on dose were evaluated.
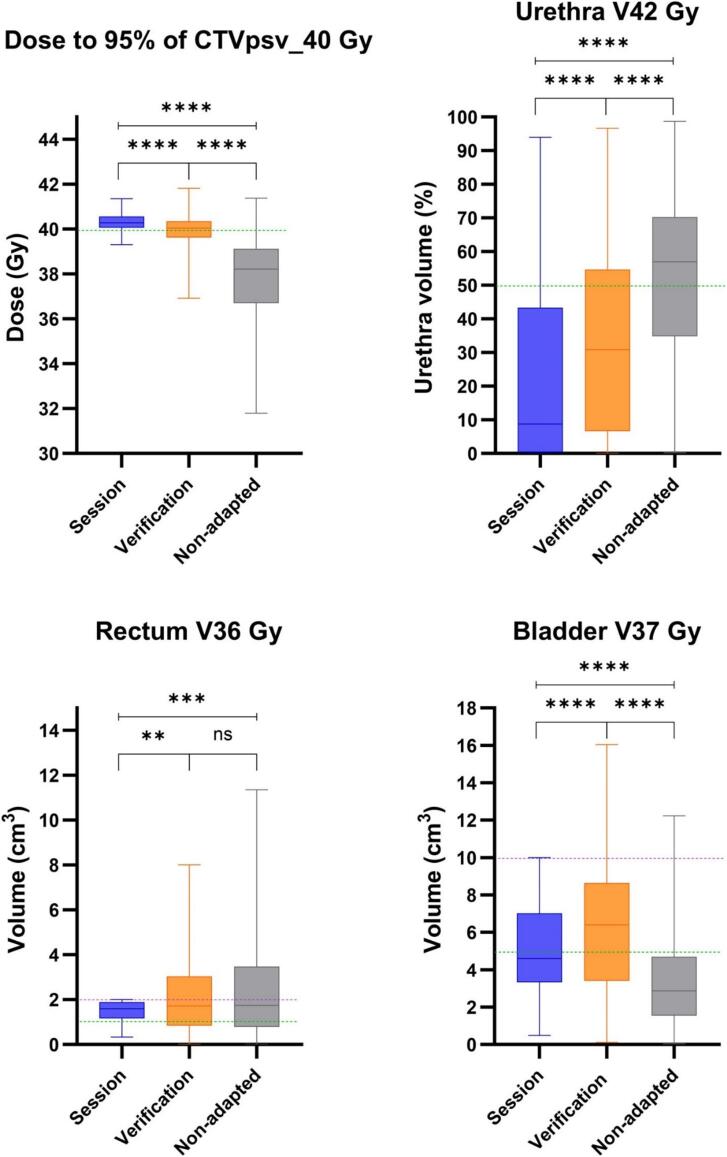
Median dose to 95 % of the CTVpsv was significantly higher with adaptation; 40.3, 40.0 and 38.2 Gy for session, verification, and non-adapted plans. Adaptation achieved a lower median urethra V42Gy dose but bladder V37Gy dose was lower when not adapting. Rectum V36Gy dose was similar for adapted and non-adapted plans.CTVpsv substructure dose difference was greatest for 1cmSV; 40.0 versus 37.5 Gy for verification/non-adapted plans. Adaptation achieved significantly higher prostate only, but not GTV doses. Prostate and rectal volume changes had a negative impact on non-adapted dose only.
MRIgART, offers significant dosimetric benefit for ultrahypofractionated prostate cancer compared to non-adapted strategies. Greatest benefit is expected for those with SV or high-risk of SV involvement, persistent rectal gas, prostate swelling and for the application of novel dose strategies including GTV dose escalation and non-involved prostate dose de-escalation.
磁共振图像引导的自适应放疗(MRIgART)通过校正每日靶区和危及器官的变形及运动来减少不确定性。与标准的图像引导非自适应放疗相比,这是第一项研究MRIgART对超分割前列腺癌治疗剂量学影响的研究。
回顾性分析了20例在Unity MR直线加速器(瑞典医科达公司)上接受超分割MRIgART的局限性前列腺癌患者。每天在线采集MRI用于重新计划(MRI),并在治疗前再采集一次用于位置验证(MRI)。为了比较有和没有自适应时的实际照射剂量,每个分次离线生成三个计划;一个疗程计划(根据MRI解剖结构调整的参考计划)、一个验证计划(在MRI解剖结构上重新计算的疗程计划)和一个非自适应计划(在MRI解剖结构上重新计算的参考计划)。计算靶区和危及器官的剂量,并评估剂量差异。二次分析使用可变形剂量累积,估计对主要靶区(CTVpsv)子结构(前列腺、大体肿瘤体积(GTV)和精囊近端1cm(1cmSV))的验证剂量和非自适应剂量。评估前列腺、直肠和膀胱体积变化对剂量的影响。
自适应时CTVpsv的95%的中位剂量显著更高;疗程计划、验证计划和非自适应计划分别为40.3、40.0和38.2Gy。自适应使尿道V42Gy剂量的中位数降低,但非自适应时膀胱V37Gy剂量更低。自适应计划和非自适应计划的直肠V36Gy剂量相似。CTVpsv子结构剂量差异在1cmSV处最大;验证/非自适应计划分别为40.0和37.5Gy。自适应仅使前列腺剂量显著更高,但GTV剂量没有显著差异。前列腺和直肠体积变化仅对非自适应剂量有负面影响。
与非自适应策略相比,MRIgART对超分割前列腺癌具有显著的剂量学益处。对于精囊受累或有精囊受累高风险、直肠持续积气、前列腺肿大以及应用包括GTV剂量递增和未受累前列腺剂量递减在内的新剂量策略的患者,预期获益最大。