Wang Yipu, Wang Gongning, Song Chao, Ma Wenqian, Zheng Xiuli, Guo Shuo, Wang Qi, Zhang Lan, Er Limian
Department of Endoscopy, The Fourth Hospital of Hebei Medical University, Shijiazhuang, Hebei, China.
The Third Department of Surgery, The Fourth Hospital of Hebei Medical University, Shijiazhuang, Hebei, China.
Front Oncol. 2025 Jun 4;15:1594591. doi: 10.3389/fonc.2025.1594591. eCollection 2025.
Gastrointestinal neuroendocrine tumor (GI-net) is a rare heterogeneous tumor, and there is a lack of models to predict its prognosis. Our study aims to develop and validate two new nomograms to predict the overall survival (OS) and cancer-specific survival (CSS) of GI-net patients and investigate their application value.
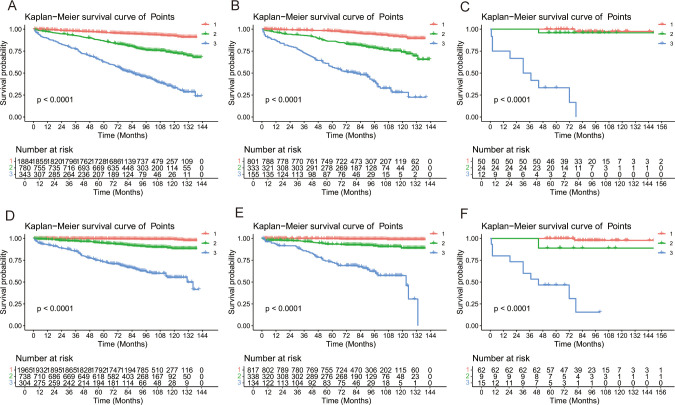
SEER*Stat 8.4.4 software was used to download clinicopathological information of GI-net patients between 2010 and 2015 from the Surveillance, Epidemiology, and End Results (SEER) database. These patients were randomly divided into a training group (n=3007) and an internal-validation group (n=1289) at a 7:3 ratio. Patients from the Fourth Hospital of Hebei Medical University were enrolled in this study to form the external-validation group (n=86). Univariate and multivariate Cox analyses were performed to explore the independent prognostic factors and establish two nomograms. The concordance index (C-index), area under the time-dependent receiver operating characteristic curve (AUC), calibration curve, and decision curve analysis (DCA) were used to evaluate the nomograms. X-tile was used to divide GI-net patients into high-, medium-, and low-risk groups. Kaplan-Meier (KM) curves and log-rank tests were used to compare survival differences among the three groups.
Seven variables (age, site, size, grade, M stage, surgery, and chemotherapy) were selected to establish the nomogram for OS, and 6 variables (age, size, grade, M stage, surgery, and chemotherapy) were selected for CSS. The C indices (0.785, 0.813, and 0.936 in the training, internal-validation, and external-validation groups for OS; 0.888, 0.893, and 0.930 for CSS, respectively) and AUCs (≥0.7) indicated that the nomograms had satisfactory discriminative ability. Calibration curve analysis and DCA revealed that the nomogram had a satisfactory ability to predict OS and CSS. KM curves indicated that each of the two nomograms clearly differentiated the high-, medium-, and low-risk groups. In addition, two online risk calculators were developed to predict the OS and CSS of these patients visually.
Our nomograms may play an important role in predicting 3- and 5-year OS and CSS for GI-net patients. Risk stratification systems and online risk calculators can be utilized in clinical practice to help doctors create personalized treatment plans.
胃肠道神经内分泌肿瘤(GI-net)是一种罕见的异质性肿瘤,目前缺乏预测其预后的模型。我们的研究旨在开发并验证两个新的列线图,以预测GI-net患者的总生存期(OS)和癌症特异性生存期(CSS),并探讨其应用价值。
使用SEER*Stat 8.4.4软件从监测、流行病学和最终结果(SEER)数据库下载2010年至2015年GI-net患者的临床病理信息。这些患者按7:3的比例随机分为训练组(n = 3007)和内部验证组(n = 1289)。河北医科大学第四医院的患者纳入本研究以形成外部验证组(n = 86)。进行单因素和多因素Cox分析以探索独立预后因素并建立两个列线图。使用一致性指数(C-index)、时间依赖性受试者工作特征曲线下面积(AUC)、校准曲线和决策曲线分析(DCA)来评估列线图。使用X-tile将GI-net患者分为高、中、低风险组。采用Kaplan-Meier(KM)曲线和对数秩检验比较三组之间的生存差异。
选择七个变量(年龄、部位、大小、分级、M分期、手术和化疗)建立OS列线图,选择六个变量(年龄、大小、分级、M分期、手术和化疗)建立CSS列线图。C指数(OS的训练组、内部验证组和外部验证组分别为0.785、0.813和0.936;CSS分别为0.888、0.893和0.930)和AUC(≥0.7)表明列线图具有令人满意的判别能力。校准曲线分析和DCA显示列线图具有令人满意的预测OS和CSS的能力。KM曲线表明两个列线图均能清晰区分高、中、低风险组。此外,还开发了两个在线风险计算器以直观地预测这些患者的OS和CSS。
我们的列线图可能在预测GI-net患者的3年和5年OS及CSS方面发挥重要作用。风险分层系统和在线风险计算器可用于临床实践,以帮助医生制定个性化治疗方案。