Wang Sheng-Yu, Gao Jia-Cheng, Wu Shuo-Dong
The Second Department of General Surgery, Shengjing Hospital of China Medical University, Shenyang 110004, Liaoning Province, China.
Department of Orthopedic Surgery, The First Hospital of China Medical University, Shenyang 110001, Liaoning Province, China.
World J Gastroenterol. 2025 Jun 7;31(21):105753. doi: 10.3748/wjg.v31.i21.105753.
Colorectal cancer has a high incidence and mortality rate, and the effectiveness of routine colonoscopy largely depends on the endoscopist's expertise. In recent years, computer-aided detection (CADe) systems have been increasingly integrated into colonoscopy to improve detection accuracy. However, while most studies have focused on adenoma detection rate (ADR) as the primary outcome, the more sensitive adenoma miss rate (AMR) has been less frequently analyzed.
To evaluate the effectiveness of CADe in colonoscopy and assess the advantages of AMR over ADR.
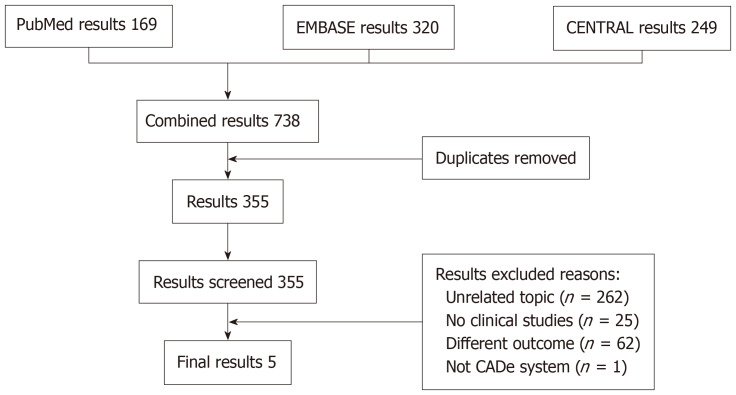
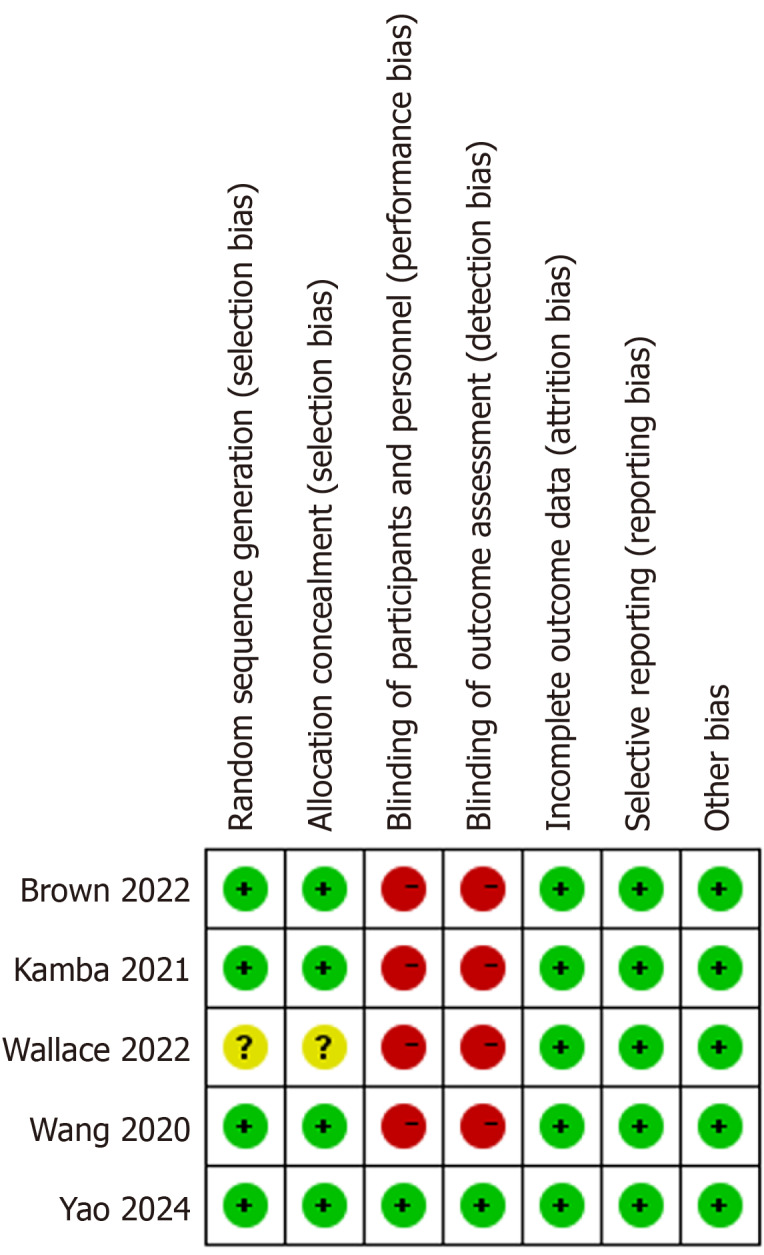
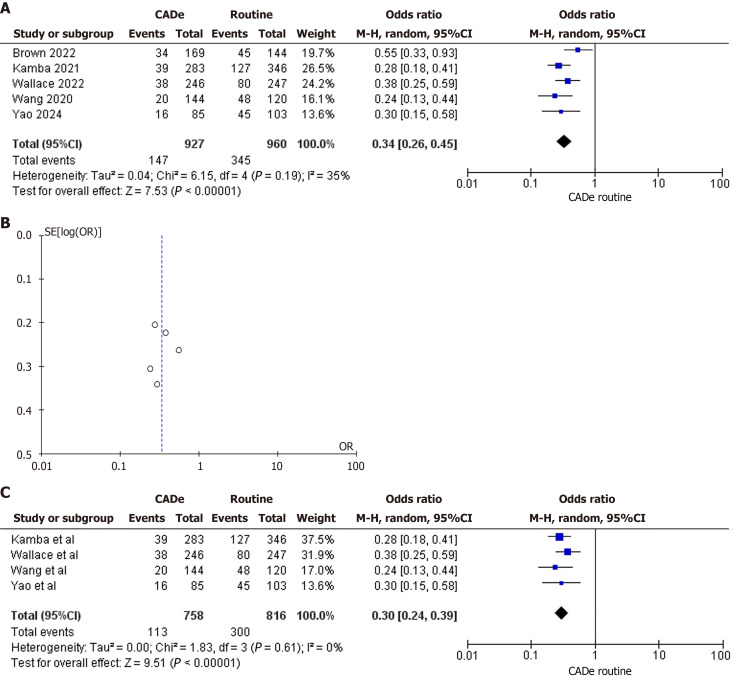
A comprehensive literature search was conducted in PubMed, Embase, and the Cochrane Central Register of Controlled Trials using predefined search strategies to identify relevant studies published up to August 2, 2024. Statistical analyses were performed to compare outcomes between groups, and potential publication bias was assessed using funnel plots. The quality of the included studies was evaluated using the Cochrane Risk of Bias tool and the Grading of Recommendations, Assessment, Development, and Evaluation approach.
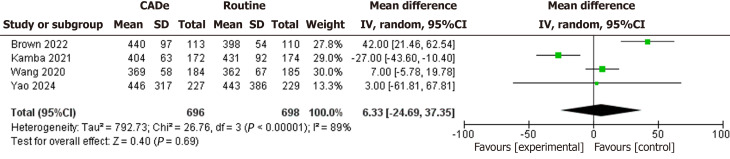
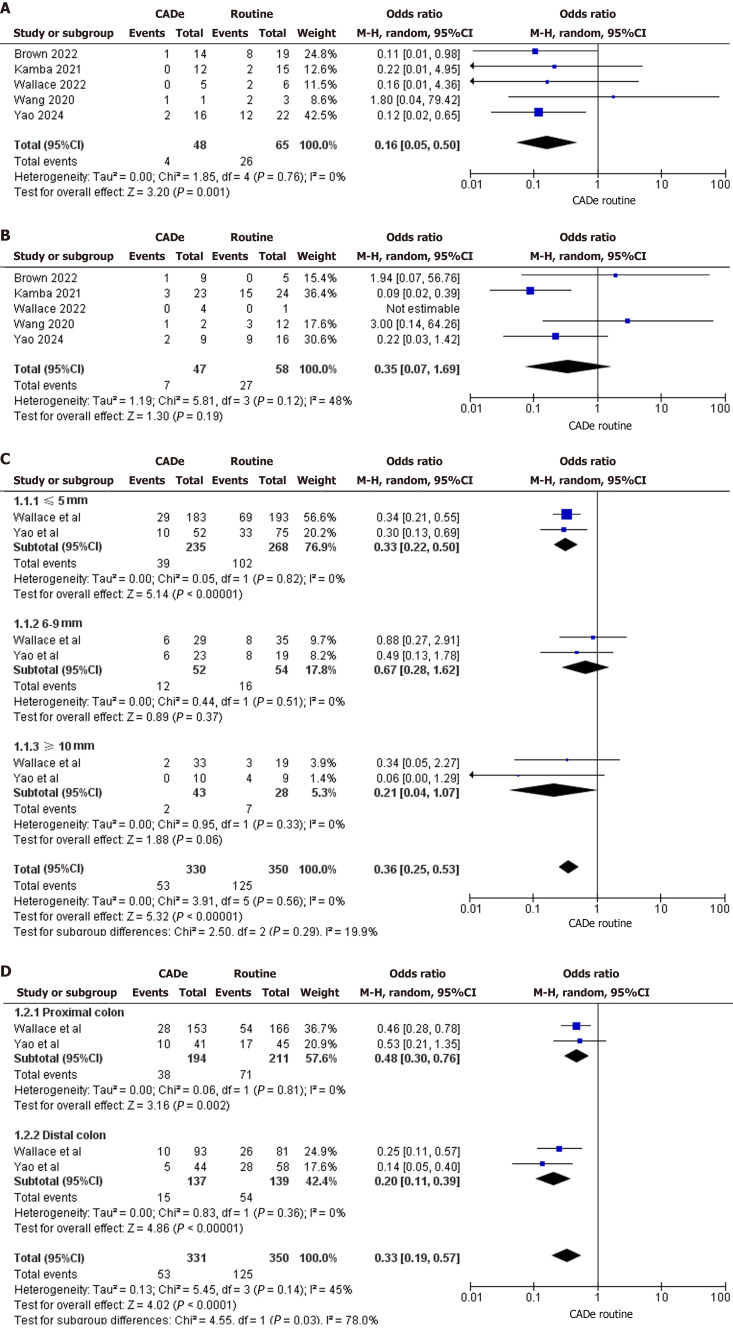
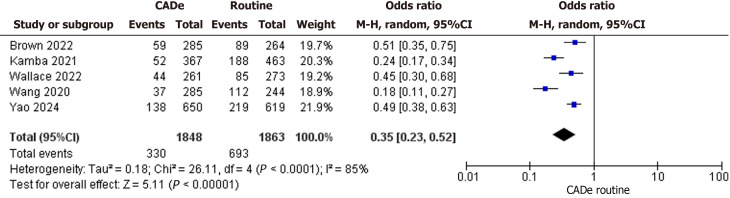
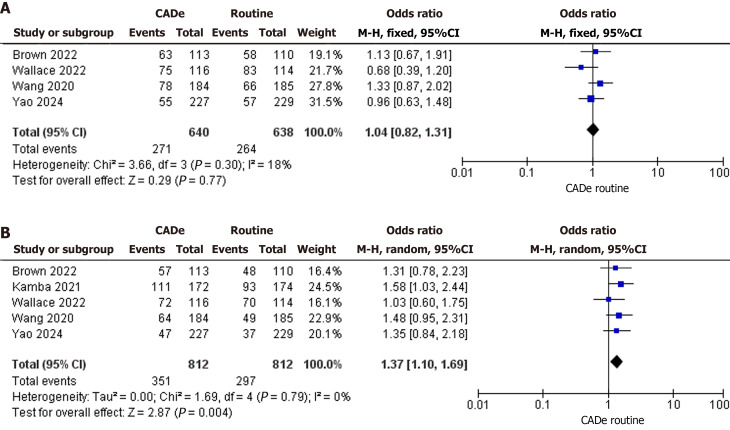
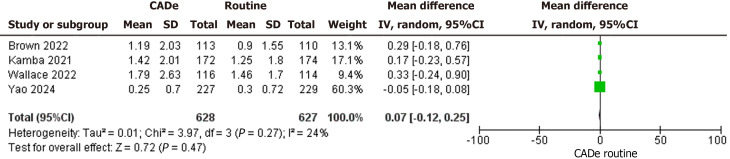
Five studies comprising 1624 patients met the inclusion criteria. AMR was significantly lower in the CADe-assisted group than in the routine colonoscopy group (147/927, 15.9% 345/960, 35.9%; < 0.01). However, CADe did not provide a significant advantage in detecting advanced adenomas or lesions measuring 6-9 mm or ≥ 10 mm. The polyp miss rate (PMR) was also lower in the CADe-assisted group [odds ratio (OR), 0.35; 95% confidence interval (CI): 0.23-0.52; < 0.01]. While the overall ADR did not differ significantly between groups, the ADR during the first-pass examination was higher in the CADe-assisted group (OR, 1.37; 95%CI: 1.10-1.69; = 0.004). The level of evidence for the included randomized controlled trials was graded as moderate.
CADe can significantly reduce AMR and PMR while improving ADR during initial detection, demonstrating its potential to enhance colonoscopy performance. These findings highlight the value of CADe in improving the detection of colorectal neoplasms, particularly small and histologically distinct adenomas.
结直肠癌发病率和死亡率较高,常规结肠镜检查的有效性很大程度上取决于内镜医师的专业水平。近年来,计算机辅助检测(CADe)系统越来越多地被整合到结肠镜检查中以提高检测准确性。然而,虽然大多数研究将腺瘤检出率(ADR)作为主要结局指标,但对更敏感的腺瘤漏诊率(AMR)的分析较少。
评估CADe在结肠镜检查中的有效性,并评估AMR相对于ADR的优势。
在PubMed、Embase和Cochrane对照试验中央注册库中进行全面的文献检索,使用预定义的检索策略识别截至2024年8月2日发表的相关研究。进行统计分析以比较组间结局,并使用漏斗图评估潜在的发表偏倚。使用Cochrane偏倚风险工具和推荐分级、评估、制定与评价方法对纳入研究的质量进行评估。
五项研究共纳入1624例患者,符合纳入标准。CADe辅助组的AMR显著低于常规结肠镜检查组(147/927,15.9% 对345/960,35.9%;P<0.01)。然而,CADe在检测高级别腺瘤或直径6 - 9 mm或≥10 mm的病变方面没有显著优势。CADe辅助组的息肉漏诊率(PMR)也较低[比值比(OR),0.35;95%置信区间(CI):0.23 - 0.52;P<0.01]。虽然两组总体ADR差异无统计学意义,但CADe辅助组首次检查时的ADR较高(OR,1.37;95%CI:1.10 - 1.69;P = 0.004)。纳入的随机对照试验的证据水平被评为中等。
CADe可显著降低AMR和PMR,同时提高初次检测时的ADR,表明其有提高结肠镜检查性能的潜力。这些发现凸显了CADe在改善结直肠肿瘤检测方面的价值,尤其是小的和组织学特征不同的腺瘤。