Wang Chengjun, Yang Chuang, Zhao Wen, Zhang Rongyu, Xuan Tiantian, Li Jisheng
Department of Medical Oncology, Qilu Hospital, Cheeloo College of Medicine, Shandong University, Jinan, Shandong, China.
Department of Medical Oncology, Qilu Hospital (Qingdao), Cheeloo College of Medicine, Shandong University, Qingdao, Shandong, China.
Front Pharmacol. 2025 Jun 9;16:1539246. doi: 10.3389/fphar.2025.1539246. eCollection 2025.
Immune checkpoint inhibitors (ICIs) combined with etoposide-platinum are recommended as the standard first-line therapy for extensive-stage small cell lung cancer (ES-SCLC). Despite the potential of antiangiogenic agents to enhance treatment efficacy, the optimal combination pattern remains unclear. This meta-analysis explores existing treatment strategies involving ICIs or antiangiogenic agents in ES-SCLC.
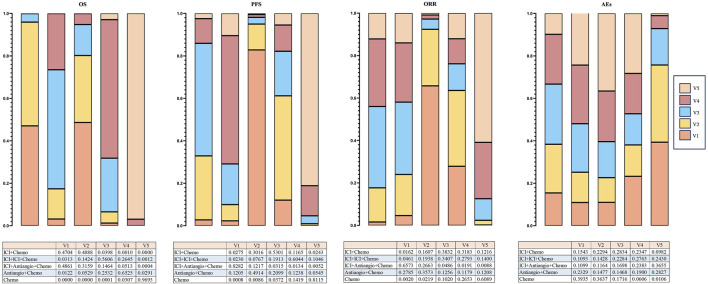
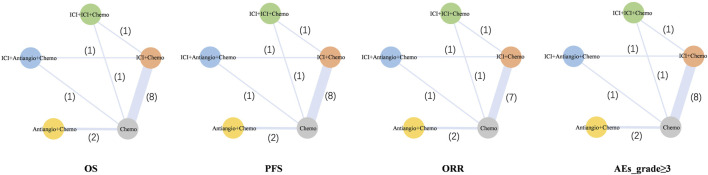
Hazard ratios (HRs) and odds ratios (ORs) were generated by R software. The outcomes of overall survival (OS), progression-free survival (PFS), objective response rate (ORR), and adverse events of grade 3 or higher (Grade ≥3 AEs) were analyzed. The included trials were classified in terms of different treatment strategies, including ICI + Chemotherapy (ICI + Chemo), ICI + ICI + Chemotherapy (ICI + ICI + Chemo), ICI + Antiangiogenic agent + Chemotherapy (ICI + Antiangio + Chemo), Antiangiogenic agent + Chemotherapy (Antiangio + Chemo), and Chemotherapy (Chemo).
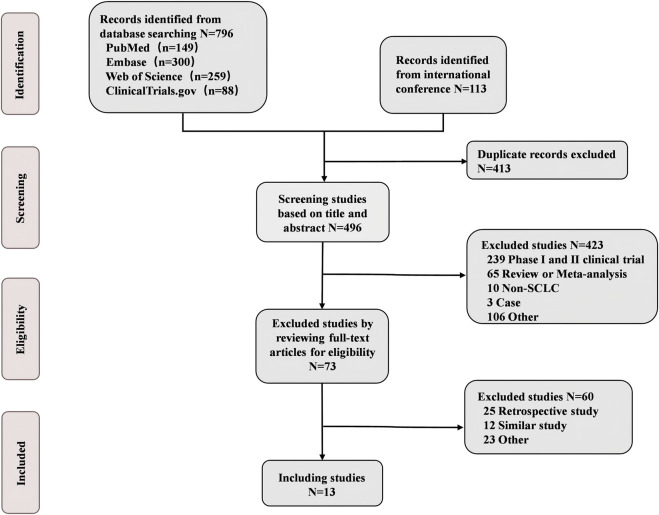
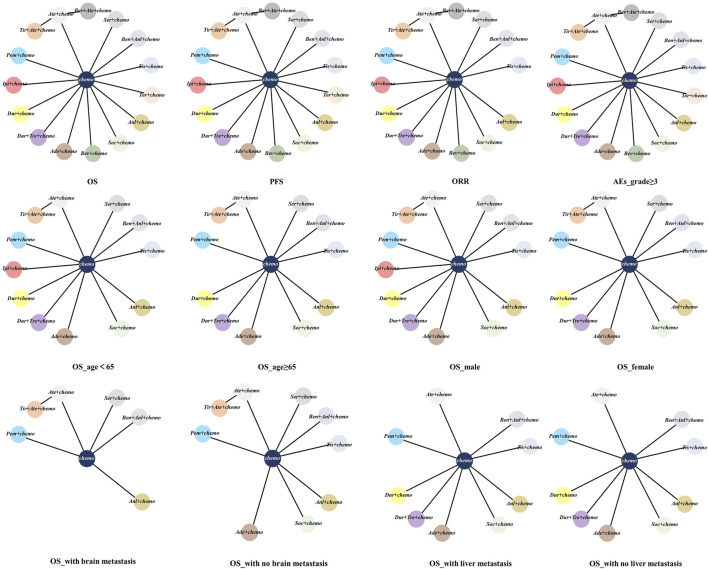
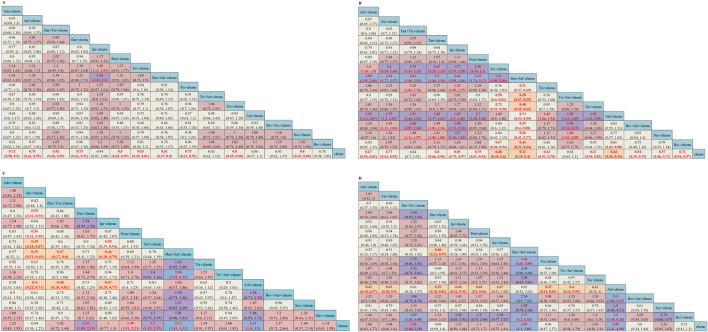
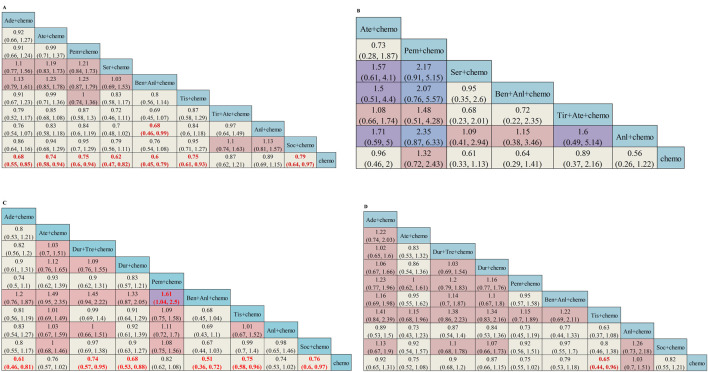
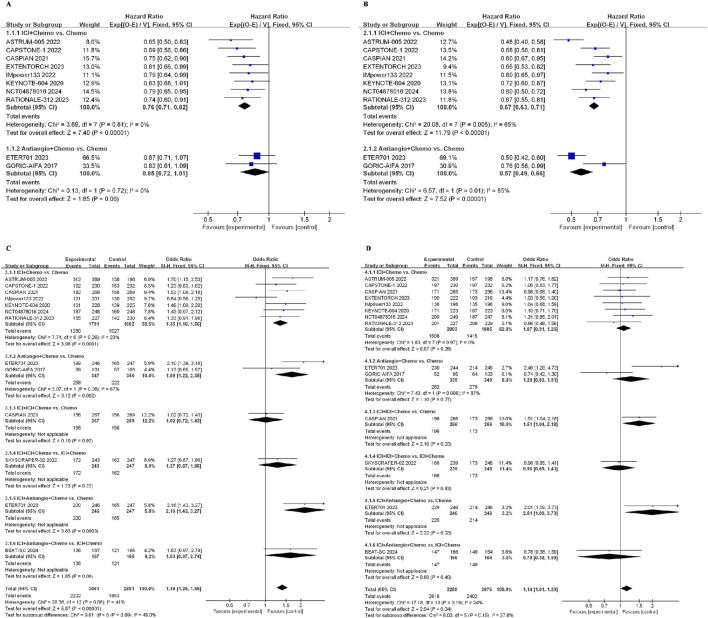
A total of 13 randomized controlled trials (RCTs) involving 6,822 patients were included in the analysis. The drug combination patterns included ipilimumab, durvalumab, adebrelimab, atezolizumab, socazolimab, pembrolizumab, serplulimab, tislelizumab, toripalimab, durvalumab + tremelimumab, tiragolumab + atezolizumab, benmelstobart + anlotinib, bevacizumab + atezolizumab, anlotinib, bevacizumab in combination with chemotherapy. The antiangiogenic agent-containing regimen benmelstobart + anlotinib + chemotherapy demonstrated the highest potential to achieve superior PFS and OS versus chemotherapy. The group meta-analysis also showed that ICI + Chemo, ICI + ICI + Chemo, and ICI + Antiangio + Chemo presented significantly better OS. Additionally, ICI + Antiangio + Chemo achieved better PFS with the lowest HR of 0.37 and the best ORR of 2.08 versus chemotherapy. Patients treated with benmelstobart + anlotinib + chemotherapy, durvalumab + tremelimumab + chemotherapy, and anlotinib + chemotherapy experienced a higher likelihood of grade ≥3 AEs.
For individuals with ES-SCLC, ICI + Antiangio + Chemo was identified as an optimal treatment option due to better OS, PFS, and ORR. Benmelstobart + anlotinib + chemotherapy demonstrated a better survival benefit than chemotherapy. The toxicity of ICI + Antiangio + Chemo was acceptable but needed careful attention. These findings clarified the roles of ICIs and antiangiogenic agent-based treatment strategies in this population.
免疫检查点抑制剂(ICIs)联合依托泊苷-铂类被推荐作为广泛期小细胞肺癌(ES-SCLC)的标准一线治疗方案。尽管抗血管生成药物有提高治疗疗效的潜力,但最佳联合模式仍不明确。本荟萃分析探讨了ES-SCLC中涉及ICIs或抗血管生成药物的现有治疗策略。
通过R软件生成风险比(HRs)和比值比(ORs)。分析总生存期(OS)、无进展生存期(PFS)、客观缓解率(ORR)以及3级或更高等级不良事件(≥3级AE)的结果。纳入的试验根据不同治疗策略进行分类,包括ICI + 化疗(ICI + Chemo)、ICI + ICI + 化疗(ICI + ICI + Chemo)、ICI + 抗血管生成药物 + 化疗(ICI + Antiangio + Chemo)、抗血管生成药物 + 化疗(Antiangio + Chemo)以及化疗(Chemo)。
分析共纳入13项涉及6822例患者的随机对照试验(RCTs)。药物联合模式包括伊匹木单抗、度伐利尤单抗、阿得贝利单抗、阿替利珠单抗、索卡利单抗、帕博利珠单抗、斯鲁利单抗、替雷利珠单抗、托瑞帕利单抗、度伐利尤单抗 + 曲美木单抗、替雷戈利单抗 + 阿替利珠单抗、苯美司他巴特 + 安罗替尼、贝伐珠单抗 + 阿替利珠单抗、安罗替尼、贝伐珠单抗联合化疗。与化疗相比,含抗血管生成药物的方案苯美司他巴特 + 安罗替尼 + 化疗在实现更好的PFS和OS方面显示出最高潜力。组间荟萃分析还表明,ICI + Chemo、ICI + ICI + Chemo和ICI + Antiangio + Chemo的OS显著更好。此外,与化疗相比,ICI + Antiangio + Chemo的PFS更好,HR最低为0.37,ORR最佳为2.08。接受苯美司他巴特 + 安罗替尼 + 化疗、度伐利尤单抗 + 曲美木单抗 + 化疗和安罗替尼 + 化疗治疗的患者发生≥3级AE的可能性更高。
对于ES-SCLC患者,由于具有更好的OS、PFS和ORR,ICI + Antiangio + Chemo被确定为最佳治疗选择。苯美司他巴特 + 安罗替尼 + 化疗显示出比化疗更好的生存获益。ICI + Antiangio + Chemo的毒性可接受,但需要密切关注。这些发现阐明了ICIs和基于抗血管生成药物的治疗策略在该人群中的作用。