Bejleri Jorin, Power Sarah, Boland Fiona, Joly Olivier, Williams David J, Thornton John J, Pfeiffer Shona
Department Physiology & Medical Physics, RCSI University of Medicine and Health Sciences, D02 YN77 Dublin, Ireland.
Department Geriatric & Stroke Medicine, Beaumont Hospital, RCSI University of Medicine and Health Sciences, D09 YD60 Dublin, Ireland.
Brain Sci. 2025 May 24;15(6):560. doi: 10.3390/brainsci15060560.
Accurate and reproducible methods for assessing infarct volume in acute ischaemic stroke have important therapeutic and prognostic implications for the choice and success of acute therapeutic interventions. However, there is no international consensus on the methodology employed in infarct volume assessment. We aimed to assess the reliability of the ABC/2 score and e-ASPECTS in the determination of infarct volume in acute ischaemic stroke.
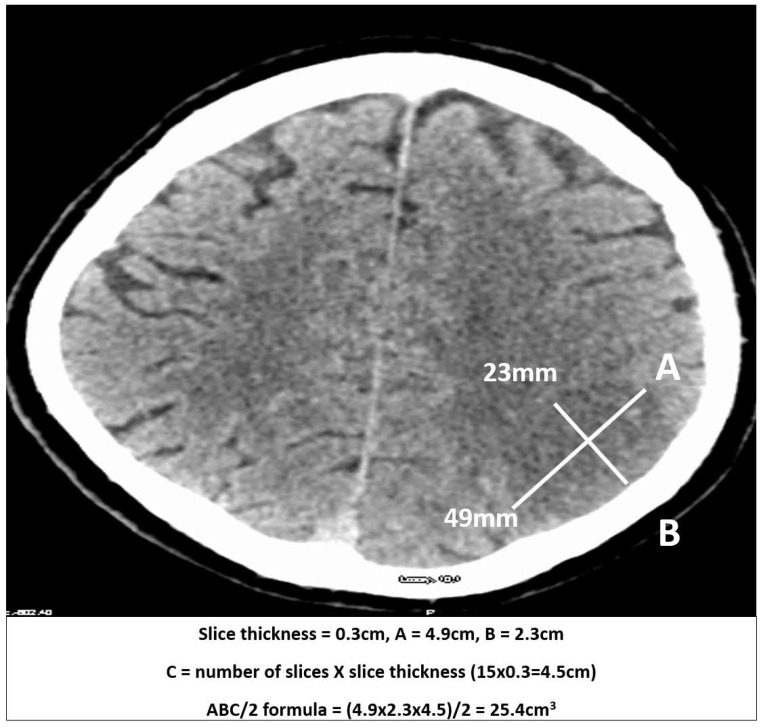
Infarct volume was measured from NCCT in stroke patients recruited ≤12 h of symptoms onset and at 24 h using the ABC/2 method. Automated ischaemic volume measurements were carried out using e-ASPECTS software. Measurements using ABC/2 were compared with e-ASPECTS to assess volume differences and reliability using Lin's concordance correlation coefficient.
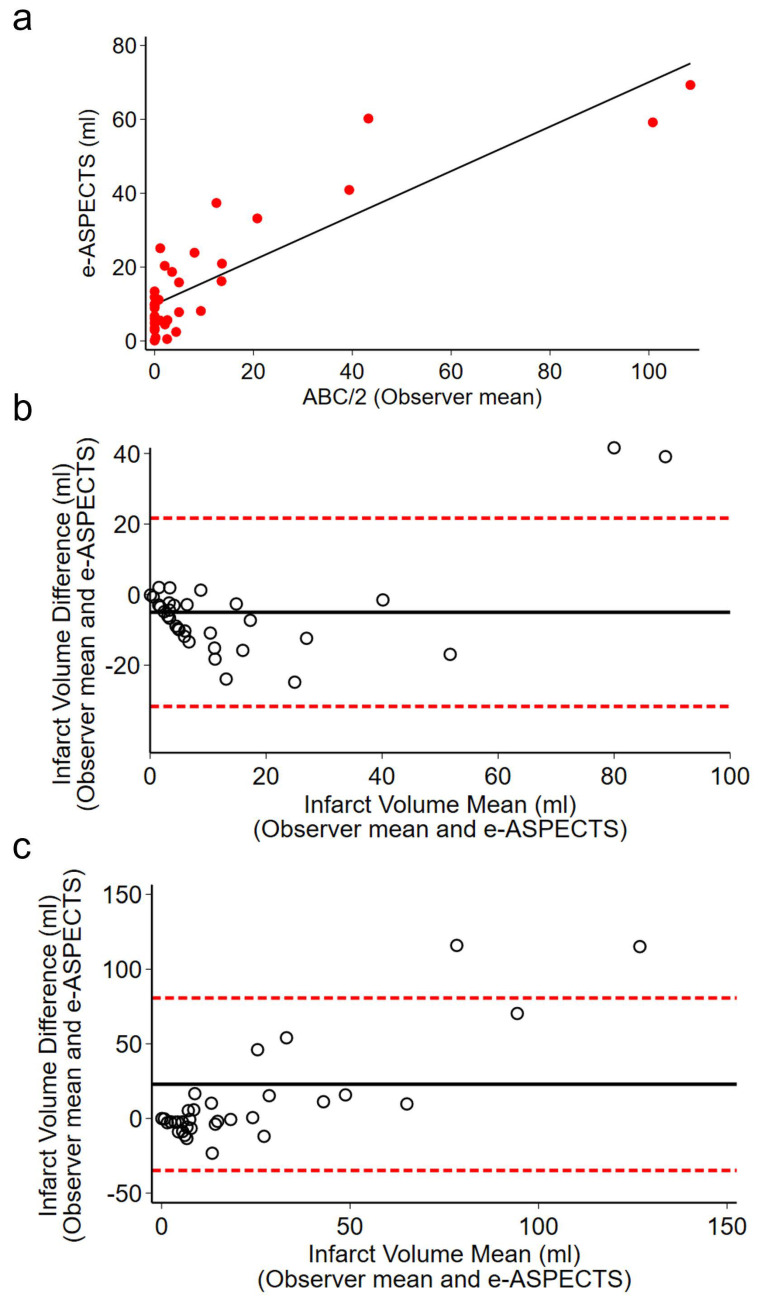
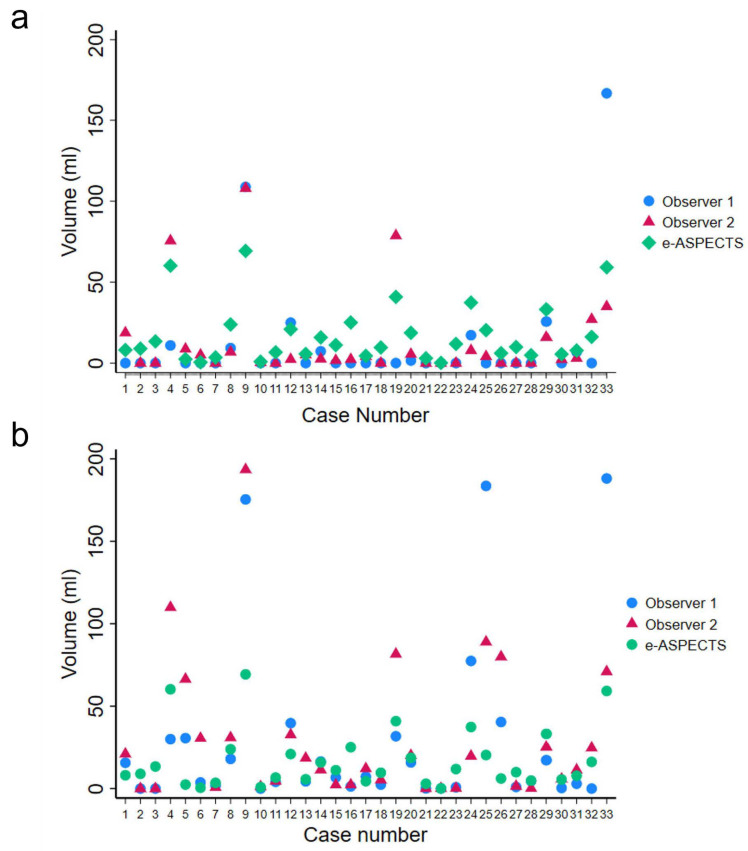
Thirty-three patients with CT < 12 h from onset of symptoms and follow-up at 24 h were included in the analysis. Use of ABC/2 demonstrated low agreement between observers (0.490, CI 0.236-0.743, < 0.001) on admission (<12 h). High agreement was found between observers at 24 h (0.724, CI 0.564-0.884, < 0.001). High agreement was observed between the mean observed infarct volumes using ABC/2 and e-ASPECTS on admission (0.794, CI 0.691-0.898, < 0.001).
Our results suggest that e-ASPECTS is a reliable platform for ischaemic volume determination particularly in the hyperacute phase to inform management. However, the use of ABC/2 represents an alternative approach to e-ASPECTS in the rapid and reliable estimation of ischaemic infarct volume to inform prognosis and treatment decisions, particularly in cases of delayed presentation where infarction is established and arterial territory boundaries are easily identifiable.
准确且可重复的急性缺血性卒中梗死体积评估方法,对于急性治疗干预措施的选择及成效具有重要的治疗和预后意义。然而,在梗死体积评估所采用的方法上,尚未达成国际共识。我们旨在评估ABC/2评分和电子ASPECTS在急性缺血性卒中梗死体积测定中的可靠性。
对症状发作≤12小时及24小时时入组的卒中患者,利用ABC/2方法从非增强CT测量梗死体积。使用电子ASPECTS软件进行自动缺血体积测量。将ABC/2测量结果与电子ASPECTS进行比较,以使用林氏一致性相关系数评估体积差异和可靠性。
分析纳入了33例症状发作后CT检查<12小时且24小时进行随访的患者。入院时(<12小时),观察者间使用ABC/2的一致性较低(0.490,CI 0.236 - 0.743,P<0.001)。24小时时观察者间一致性较高(0.724,CI 0.564 - 0.884,P<0.001)。入院时,使用ABC/2和电子ASPECTS测得的平均梗死体积间一致性较高(0.794,CI 0.691 - 0.898,P<0.001)。
我们的结果表明,电子ASPECTS是用于缺血体积测定的可靠平台,尤其在超急性期可指导治疗。然而,在快速且可靠地估计缺血性梗死体积以指导预后和治疗决策方面,ABC/2的使用是电子ASPECTS的一种替代方法,特别是在梗死已确定且动脉供血区边界易于识别的延迟就诊病例中。