Han Soo Hyun, Kang Changshin, Park Hyerim, Lee Eu Jin, Ham Young Rok, Na Ki Ryang, Park Jung Soo, Choi Dae Eun
Department of Nephrology, College of Medicine, Chungnam National University, 266 Munwha-ro, Jung-gu, Daejeon 35015, Republic of Korea.
Department of Emergency Medicine, Chungnam National University Hospital, 282 Munwha-ro, Jung-gu, Daejeon 35015, Republic of Korea.
Life (Basel). 2025 May 27;15(6):866. doi: 10.3390/life15060866.
The impact of initial emergency room (ER) factors on survival and renal function in critically ill patients undergoing continuous renal replacement therapy (CRRT) remains unclear. This study aimed to evaluate whether these initial factors influence survival and renal recovery in such patients.
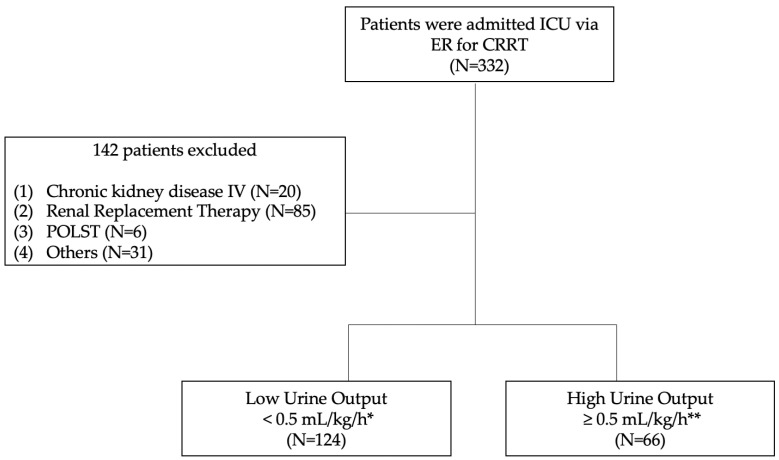
This single-center, retrospective study included 190 critically ill patients admitted to the intensive care unit (ICU) via the ER for CRRT between 1 March 2018, and 31 May 2021. Clinical parameters, including urine output, estimated glomerular filtration rate (eGFR), and serum neutrophil gelatinase-associated lipocalin (NGAL), were assessed. The primary outcomes were 30-day and 90-day mortality, while secondary outcomes included 30-day and 90-day RRT-free durations.
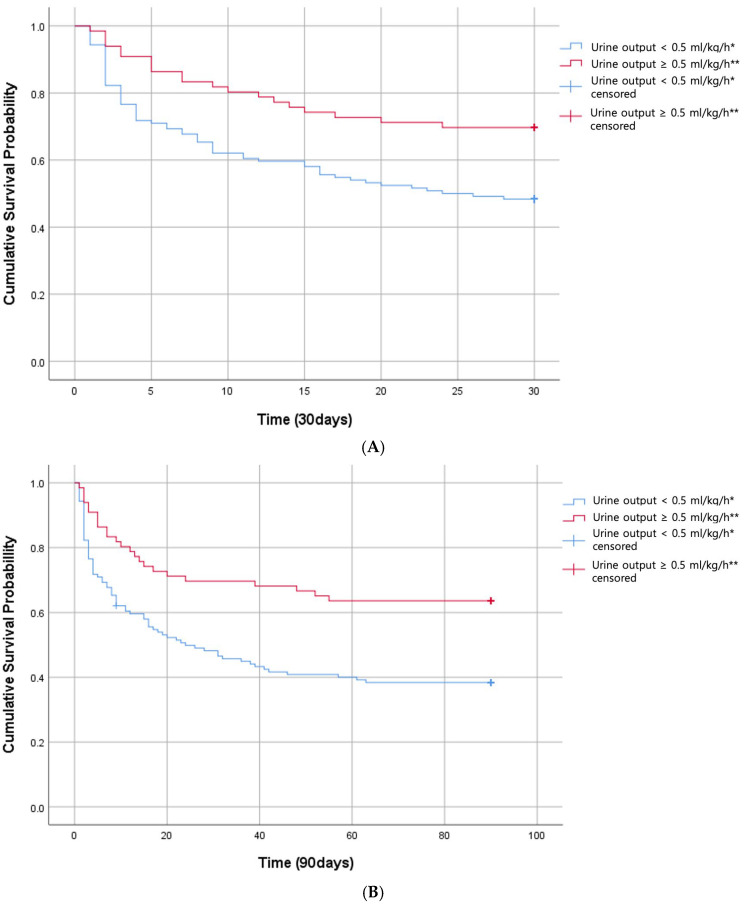
Patients with low urine output (LUO, defined as the average of <0.5 mL/kg/h over 6 h) were significantly associated with higher 30-day and 90-day mortality rates. Multivariable Cox regression analysis revealed that the LUO group had an increased risk of 30-day and 90-day mortality (hazard ratios: 1.935 and 2.141, respectively) compared to the high urine output (HUO, defined as the average of ≥0.5 mL/kg/h over 6 h) group. No significant association was observed between mortality and initial eGFR or plasma NGAL levels. However, the HUO group and patients with initial eGFR ≥ 30 mL/min/1.73 m had longer RRT-free durations at 30 and 90 days. Plasma NGAL levels did not significantly correlate with RRT-free durations.
Initial 6-h urine output in the ER is a significant predictor of 30-day and 90-day mortality in critically ill patients undergoing CRRT.
初始急诊室(ER)因素对接受持续肾脏替代治疗(CRRT)的危重症患者生存及肾功能的影响尚不清楚。本研究旨在评估这些初始因素是否影响此类患者的生存及肾脏恢复情况。
本单中心回顾性研究纳入了2018年3月1日至2021年5月31日期间经急诊室收入重症监护病房(ICU)接受CRRT的190例危重症患者。评估了包括尿量、估算肾小球滤过率(eGFR)及血清中性粒细胞明胶酶相关脂质运载蛋白(NGAL)在内的临床参数。主要结局为30天及90天死亡率,次要结局包括30天及90天无肾脏替代治疗(RRT)持续时间。
少尿(LUO,定义为6小时内平均<0.5 mL/kg/h)患者与30天及90天死亡率显著相关。多变量Cox回归分析显示,与高尿量(HUO,定义为6小时内平均≥0.5 mL/kg/h)组相比,LUO组30天及90天死亡风险增加(风险比分别为1.935和2.141)。未观察到死亡率与初始eGFR或血浆NGAL水平之间存在显著关联。然而,HUO组及初始eGFR≥30 mL/min/1.73 m²的患者在30天和90天时无RRT持续时间更长。血浆NGAL水平与无RRT持续时间无显著相关性。
急诊室初始6小时尿量是接受CRRT的危重症患者30天和90天死亡率的重要预测指标。