Weng Bob, Braaten Marco, Lehn Jenna, Morrissey Reid, Asghar Muhammad Sohaib, Silberstein Peter, Abdul Jabbar Ali Bin, Mathews Abraham, Tauseef Abubakar, Mirza Mohsin
Department of Internal Medicine, Creighton University School of Medicine, Omaha, NE 68178, United States.
Division of Nephrology and Hypertension, Mayo Clinic, Rochester, MN 55905, United States.
World J Nephrol. 2025 Jun 25;14(2):103923. doi: 10.5527/wjn.v14.i2.103923.
Renal cell carcinoma (RCC) is treated with surgical resection as the gold standard, as it is notoriously resistant to systemic therapy. Advancements with targeted therapies contribute to declining mortality, but metastatic RCC (mRCC) survival remains poor. One possible factor is treatment at academic centers, which employ advanced providers and novel therapies. This study compared outcomes of mRCC in patients treated at academic/research facilities compared to those treated at non-academic centers.
To compare survival outcomes of mRCC and their various etiologies between academic and non-academic centers.
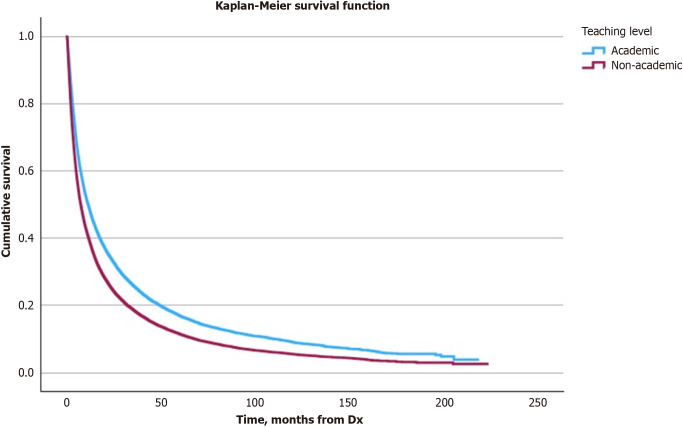
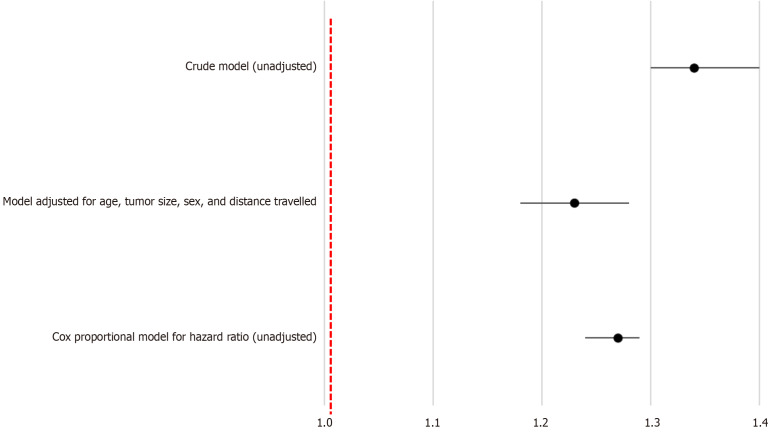
The National Cancer Database was used to identify mRCC patients including all histology subtypes and stage IV disease. Descriptive statistics and Kaplan-Meier curves measured survival outcomes for user file facility types sorted into a binary academic/research and non-academic research variable. Multivariate logistic regression and Cox proportional hazard testing generated odds ratio and hazard ratio. Data was analyzed using Statistical Package for the Social Sciences version 29.0 using a significance level of < 0.05.
Overall, academic facility patients experienced greater 5-year and 10-year overall survival than non-academic facility patients. Treatment at non-academic facilities was associated with increased odds of death that persisted even after controlling for age, tumor size, sex, and distance traveled to treatment center. In comparison, non-academic facility patients also experienced greater risk of hazard.
Patients with mRCC treated at academic/research facilities experienced increased survival compared to patients treated at non-academic facilities, were more likely to be younger, carry private insurance, and come from a large metropolitan area. They also were significantly more likely to receive surgery and adjuvant immunotherapy.
肾细胞癌(RCC)的治疗以手术切除为金标准,因为它对全身治疗具有众所周知的耐药性。靶向治疗的进展有助于降低死亡率,但转移性肾细胞癌(mRCC)的生存率仍然很低。一个可能的因素是在学术中心接受治疗,这些中心拥有先进的医疗人员和新型疗法。本研究比较了在学术/研究机构接受治疗的mRCC患者与在非学术中心接受治疗的患者的结局。
比较学术中心和非学术中心mRCC患者的生存结局及其各种病因。
使用国家癌症数据库识别mRCC患者,包括所有组织学亚型和IV期疾病。描述性统计和Kaplan-Meier曲线测量了按学术/研究和非学术研究二元变量分类的用户档案机构类型的生存结局。多变量逻辑回归和Cox比例风险测试生成比值比和风险比。使用社会科学统计软件包第29.0版分析数据,显著性水平<0.05。
总体而言,学术机构的患者比非学术机构的患者有更高的5年和10年总生存率。在非学术机构接受治疗与死亡几率增加相关,即使在控制了年龄、肿瘤大小、性别和前往治疗中心的距离后,这种相关性仍然存在。相比之下,非学术机构的患者也有更高的风险。
与在非学术机构接受治疗的患者相比,在学术/研究机构接受治疗的mRCC患者生存率更高,更可能年轻、拥有私人保险且来自大城市地区。他们也更有可能接受手术和辅助免疫治疗。