Kuguyo Oppah, Mancitshana Lindiwe, Mangenah Collin, Tumushime Mary K, Ruhode Nancy, Matsikire Edward, Kalweo Jane, Terris-Prestholt Fern, Cowan Frances M, Sibanda Euphemia Lindelwe
Centre for Sexual Health and HIV/AIDS Research (CeSHHAR), Harare, Zimbabwe.
Department of International Public Health, Liverpool School of Tropical Medicine, Liverpool, UK.
J Int AIDS Soc. 2025 Jun;28 Suppl 1(Suppl 1):e26461. doi: 10.1002/jia2.26461.
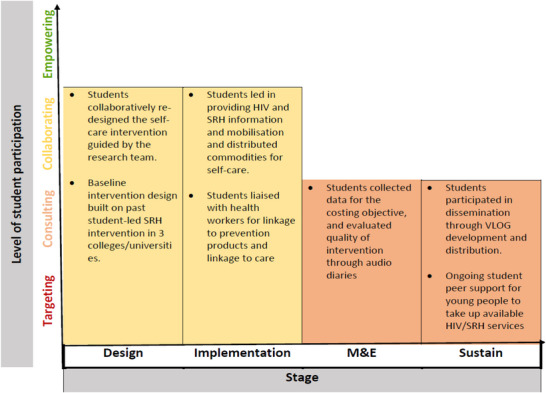
There is a growing appreciation that community-led interventions are key to sustaining the HIV response and achieving HIV prevention and treatment targets. Together with young people in colleges/universities and Ministry of Health (MOH), we developed and evaluated a student-led intervention for promoting the uptake of HIV self-testing (HIVST), post-exposure prophylaxis (PEP) and emergency contraception (EC) among college/university students.
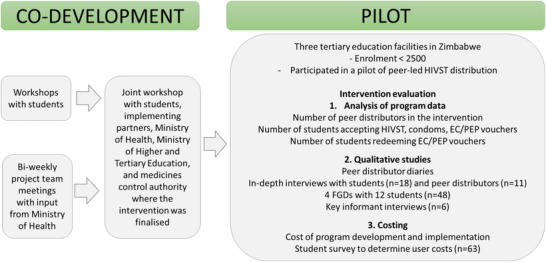
Over 3 months, in biweekly study team meetings, two workshops with students, two meetings with MOH, and a joint workshop with students, MOH and relevant stakeholders, we co-developed an intervention for peer-led promotion/distribution of HIVST, PEP, EC and condoms. The agreed intervention was piloted in three Zimbabwean colleges/universities from December 2023 to February 2024. Student peers distributed HIVST and condoms directly, and vouchers for PEP and EC that were redeemed at college/nearby clinics. During co-development, students strongly preferred peer distribution of all commodities but this was restricted by regulatory requirements for PEP and EC. Peer distributors (n = 14) kept daily audio diaries of their experiences. In-depth interviews were held with students (n = 18), peer distributors (n = 11) and key informants (n = 12) to explore views/preferences, with participant observations and four focus group discussions to provide additional insights. We determined the intervention development and implementation costs.
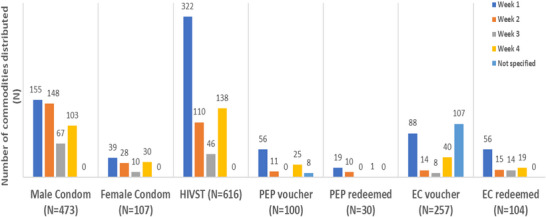
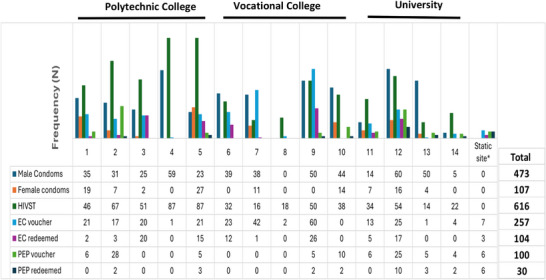
Peer-led distribution of HIVST, PEP and EC to college/university students was acceptable, feasible, appropriate and generally implemented as intended. PEP and EC acceptability was driven by high HIV and pregnancy risk among students, who had no easy access to services. Of 100 PEP and 257 EC vouchers distributed, 30% and 40% were redeemed, respectively. The main barrier to PEP and EC uptake was moral judgement against premarital sex, which affected female students more. Judgemental health worker attitudes also limited uptake of PEP and EC. EC voucher redemption among female students was lower versus males, aOR = 0.4 (95% CI = 0.2-0.8), p = 0.019. Redemption was also higher at the college where the nearby clinic could be accessed discreetly. Total cost of the intervention per student was $14.57 (cross-institution range: $7.26-$35.52).
Student-led distribution of HIVST, PEP and EC was feasible, acceptable and affordable. Making the intervention more community-driven according to the 2024 WHO PEP guidelines will likely achieve great impact.
人们越来越认识到,社区主导的干预措施是维持艾滋病应对工作以及实现艾滋病预防和治疗目标的关键。我们与高校学生及卫生部共同开发并评估了一项由学生主导的干预措施,以促进高校学生接受艾滋病自我检测(HIVST)、暴露后预防(PEP)和紧急避孕(EC)。
在3个多月的时间里,通过每两周一次的研究团队会议、两次与学生的工作坊、两次与卫生部的会议以及一次与学生、卫生部和相关利益攸关方的联合工作坊,我们共同开发了一项由同伴主导的促进/分发HIVST、PEP、EC和避孕套的干预措施。商定的干预措施于2023年12月至2024年2月在津巴布韦的三所高校进行试点。学生同伴直接分发HIVST和避孕套,以及用于PEP和EC的代金券,这些代金券可在学校/附近诊所兑换。在共同开发过程中,学生强烈倾向于由同伴分发所有商品,但这受到PEP和EC监管要求的限制。同伴分发者(n = 14)每天记录他们的经历音频日记。对学生(n = 18)、同伴分发者(n = 11)和关键信息提供者(n = 12)进行了深入访谈,以探讨他们的观点/偏好,并通过参与观察和四次焦点小组讨论提供更多见解。我们确定了干预措施的开发和实施成本。
由同伴主导向高校学生分发HIVST、PEP和EC是可接受的、可行的、适当的,并且总体上按计划实施。学生中较高的艾滋病和怀孕风险以及难以获得相关服务,推动了对PEP和EC的接受。在分发的100份PEP和257份EC代金券中,分别有30%和40%被兑换。接受PEP和EC的主要障碍是对婚前性行为的道德评判,这对女学生的影响更大。医务人员的评判态度也限制了PEP和EC的接受。女学生的EC代金券兑换率低于男学生,调整后的比值比(aOR) = 0.4(95%置信区间 = 0.2 - 0.8),p = 0.019。在附近诊所可以谨慎就诊的学校,兑换率也更高。每名学生的干预总成本为14.57美元(跨机构范围:7.26 - 35.52美元)。
由学生主导分发HIVST、PEP和EC是可行的、可接受的且成本低廉。根据2024年世界卫生组织PEP指南,使干预措施更具社区驱动性可能会产生巨大影响。