Papanikolaou Vicki, Goh Ethan, Carrandi Alayna, Charles-Nelson Anaïs, Kottakkal Kiran, Romero Lorena, Hodgson Carol L, Higgins Alisa M
Australian and New Zealand Intensive Care Research Centre, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia.
Alfred Health, Melbourne, Victoria, Australia.
CJC Open. 2025 Mar 31;7(6):750-758. doi: 10.1016/j.cjco.2025.03.019. eCollection 2025 Jun.
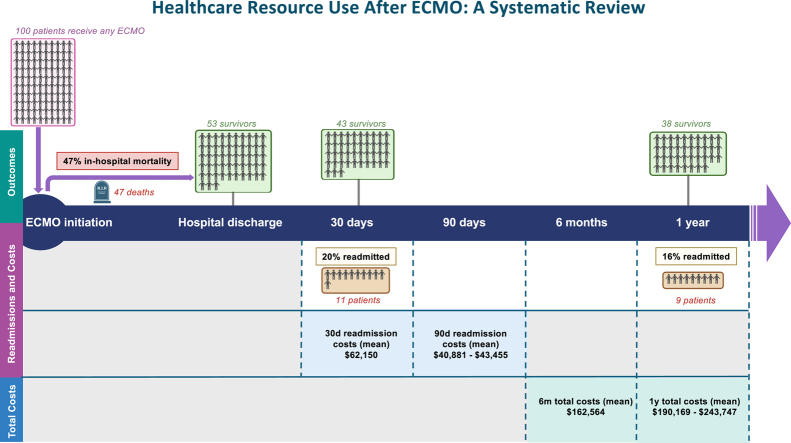
Extracorporeal membrane oxygenation (ECMO) is a high-cost, resource-intensive intervention for severe cardiac and respiratory failure. Survivors of ECMO have healthcare needs that extend beyond their acute hospitalization, placing significant demands on healthcare systems and society. As ECMO use increases globally, understanding the healthcare and economic burden of ECMO survivorship is needed to improve long-term outcomes of ECMO survivors and optimize resource allocation within healthcare systems.
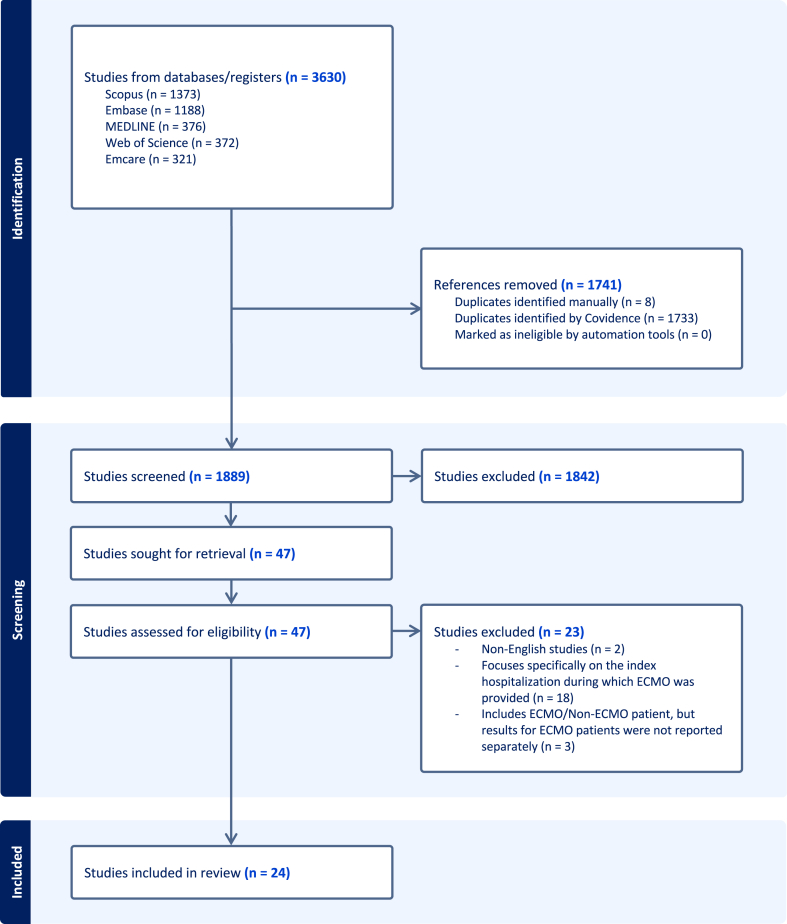
We systematically searched Ovid MEDLINE, Ovid Embase, Ovid Emcare, Scopus, and Web of Science from inception to October 1, 2024. We included studies published in English that reported post-discharge healthcare resource utilization and costs for adult survivors of ECMO.
From 1889 articles screened, 24 studies met our inclusion criteria. Most were retrospective cohort studies conducted in North America between 2010 and 2024. Sample sizes ranged from 12 to 23,876 patients, with in-hospital mortality rates between 28.5% and 67.4%. Thirty-day readmission rates ranged from 10.0% to 43.8%, with 90-day rates ranging from 21.1% to 53.0%. One study reported a mean 30-day readmission cost of $62,150 (in 2023 US dollars). Only 5 studies (20.8%) reported total healthcare costs up to 6 months and 1 year.
ECMO survivorship is gaining increased attention in research and clinical practice, yet significant gaps remain in our understanding of long-term healthcare resource utilization and costs. Our review reveals very limited information, indicating an urgent need for more comprehensive and granular data to guide clinical and policy decisions and achieve healthcare system efficiency.
体外膜肺氧合(ECMO)是一种针对严重心脏和呼吸衰竭的高成本、资源密集型干预措施。ECMO幸存者的医疗保健需求超出了急性住院期间,给医疗系统和社会带来了巨大需求。随着全球ECMO使用的增加,需要了解ECMO幸存者的医疗保健和经济负担,以改善ECMO幸存者的长期预后,并优化医疗系统内的资源分配。
我们系统检索了从创刊至2024年10月1日的Ovid MEDLINE、Ovid Embase、Ovid Emcare、Scopus和Web of Science数据库。我们纳入了以英文发表的研究,这些研究报告了ECMO成年幸存者出院后的医疗资源利用情况和费用。
在筛选的1889篇文章中,有24项研究符合我们的纳入标准。大多数是2010年至2024年在北美进行的回顾性队列研究。样本量从12例到23876例患者不等,住院死亡率在28.5%至67.4%之间。30天再入院率在10.0%至43.8%之间,90天再入院率在21.1%至53.0%之间。一项研究报告,30天再入院的平均费用为62150美元(2023年美元)。只有5项研究(20.8%)报告了长达6个月和1年的总医疗费用。
ECMO幸存者在研究和临床实践中越来越受到关注,但我们对长期医疗资源利用和费用的理解仍存在重大差距。我们的综述显示信息非常有限,表明迫切需要更全面、更详细的数据来指导临床和政策决策,并提高医疗系统效率。