Guo Lan-Wei, Lyu Zhang-Yan, Liu Yin, Meng Qing-Cheng, Zheng Li-Yang, Chen Qiong, Xu Hui-Fang, Kang Rui-Hua, Liu Shu-Zheng, Zhang Shao-Kai
Department of Cancer Epidemiology and Prevention, Henan Engineering Research Center of Cancer Prevention and Control, Henan Cancer Hospital, Henan International Joint Laboratory of Cancer Prevention, The Affiliated Cancer Hospital of Zhengzhou University, Dongming Road No. 127, PO Box 0061, Zhengzhou, 450008, China.
Department of Cancer Epidemiology and Biostatistics, Key Laboratory of Cancer Prevention and Therapy of Tianjin, Tianjin's Clinical Research Center for Cancer, Key Laboratory of Molecular Cancer Epidemiology of Tianjin, Key Laboratory of Breast Cancer Prevention and Therapy of the Ministry of Education, Tianjin Medical University Cancer Institute and Hospital, National Clinical Research Center for Cancer, Tianjin, China.
BMC Cancer. 2025 Jul 1;25(1):1058. doi: 10.1186/s12885-025-14449-6.
Low dose computed tomography (LDCT) screening has been proven to be effective in reducing lung cancer mortality, but the ensuing high false-positive and overdiagnosis rates shackle the effectiveness of lung cancer screening (LCS) in China. Nodule malignancy prediction models may be an applicable solution.
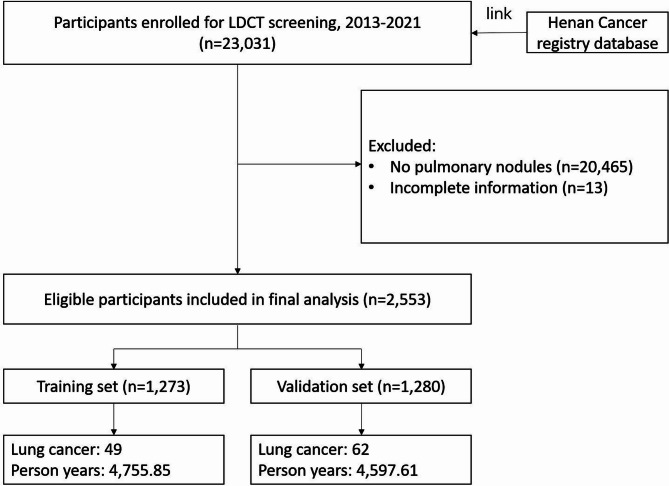
We conducted a prospective cohort study to develop and internally validate the model using data from the ongoing Henan province Cancer Screening Program in Urban China (CanSPUC). From 2013 to 2021, 23,031 heavy smokers underwent baseline screening with LDCT; 2553 participants were diagnosed with pulmonary nodules. Detailed questionnaire, physical assessment and follow-up were completed for all participants. Multivariable Cox proportional risk regression models were used to identify and integrate key prognostic factors for the development of a nomogram model. Data from the National Lung Screening Trial (NLST) were utilized for external validation.
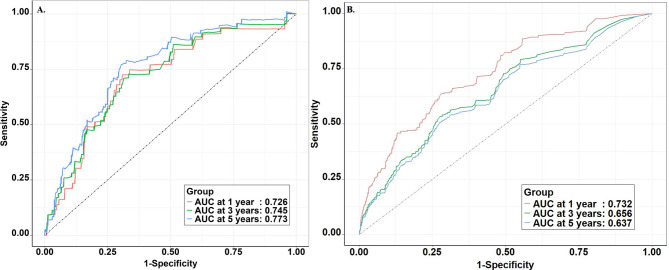
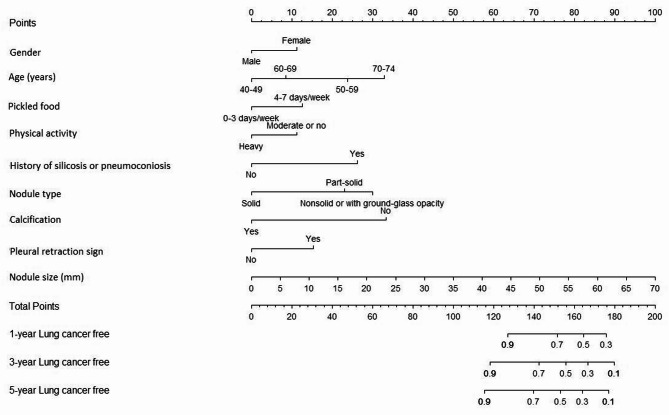
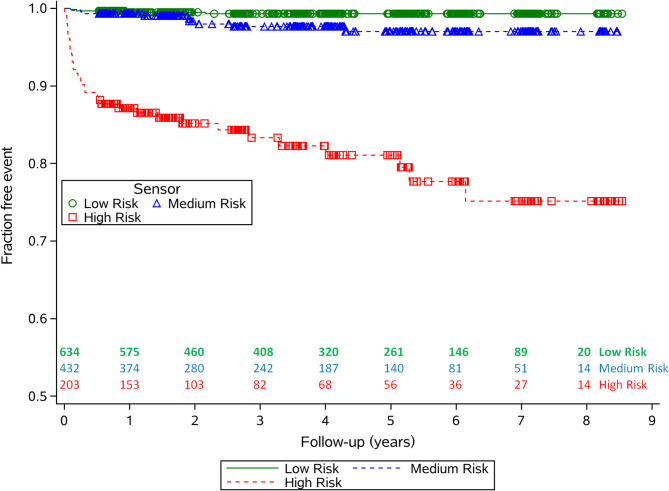
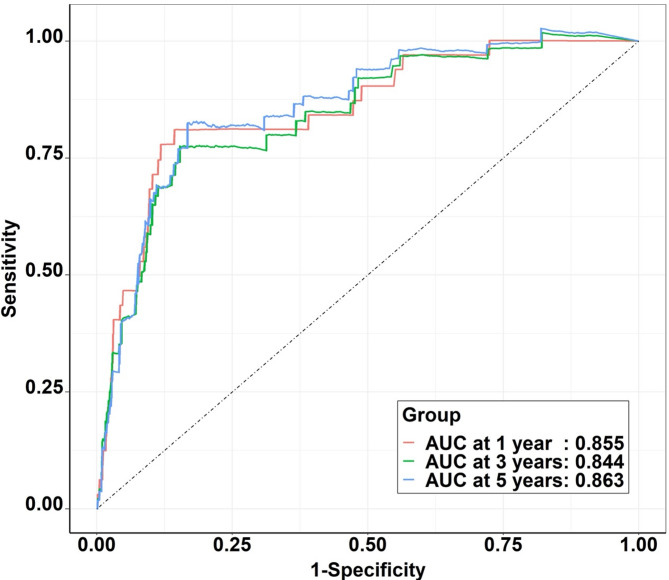
A total of 111 lung cancer cases with a median follow-up duration of 3.7 years occurred in the Henan CanSPUC. Age, gender, physical activity, consumption of pickled food, history of silicosis or pneumoconiosis, nodule type, size, calcification, and pleural retraction sign were included into the model. The AUC was 0.855, 0.844, and 0.863 for the 1-, 3- and 5-year lung cancer risk in the training set, respectively. Compared with Mayo model, VA model, PKU model, and Brock model, the Henan CanSPUC model yield statistically better discriminatory performance (all P values < 0.05). The model calibrated well across the deciles of predicted risk in both the overall population and all subgroups. The model demonstrated good calibration and discrimination in the internal validation cohort, while the external validation cohort showed lower predictive performance, indicating that further external validation is needed.
The model developed and validated in this study may be used to estimate the probability of lung cancer in nodules detected at baseline LDCT, allowing more efficient risk-adapted follow-up in population-based LCS programs. However, further external validation in broader and more diverse populations is warranted.
低剂量计算机断层扫描(LDCT)筛查已被证明可有效降低肺癌死亡率,但随之而来的高假阳性率和过度诊断率限制了中国肺癌筛查(LCS)的有效性。结节恶性预测模型可能是一个适用的解决方案。
我们进行了一项前瞻性队列研究,使用来自中国河南省城市癌症筛查项目(CanSPUC)的现有数据来开发并内部验证该模型。2013年至2021年期间,23,031名重度吸烟者接受了LDCT基线筛查;2553名参与者被诊断出患有肺结节。对所有参与者完成了详细的问卷调查、体格检查及随访。使用多变量Cox比例风险回归模型来识别并整合关键预后因素,以建立列线图模型。来自国家肺癌筛查试验(NLST)的数据用于外部验证。
在河南CanSPUC队列中,共发生111例肺癌病例,中位随访时间为3.7年。纳入模型的因素包括年龄、性别、体力活动、腌制食品摄入量、矽肺或尘肺病史、结节类型、大小、钙化及胸膜凹陷征。训练集中1年、3年和5年肺癌风险的AUC分别为0.855、0.844和0.863。与梅奥模型、VA模型、北大模型和布罗克模型相比,河南CanSPUC模型具有统计学上更好的区分性能(所有P值<0.05)。该模型在总体人群和所有亚组的预测风险十分位数中校准良好。该模型在内部验证队列中显示出良好的校准和区分能力,而外部验证队列的预测性能较低,表明需要进一步进行外部验证。
本研究中开发并验证的模型可用于估计在基线LDCT检测到的结节中患肺癌的概率,从而在基于人群的LCS项目中实现更有效的风险适应性随访。然而,有必要在更广泛和更多样化的人群中进一步进行外部验证。