Wang Jiali, Liu Jia, Lin Qingsong, Zhang Fengkui, Zheng Yizhou, Xiao Zhijian, Wang Jianxiang, Pang Aiming, He Yi, Jiang Erlie, Feng Sizhou, Han Mingzhe, Zhai Weihua
State Key Laboratory of Experimental Hematology, National Clinical Research Center for Blood Diseases, Haihe Laboratory of Cell Ecosystem, Institute of Hematology & Blood Diseases Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Tianjin, China.
Tianjin Institutes of Health Science, Tianjin, China.
Front Cell Infect Microbiol. 2025 Jun 17;15:1600746. doi: 10.3389/fcimb.2025.1600746. eCollection 2025.
Carbapenem-resistant Enterobacterales (CRE) bloodstream infections (BSI) represent a frequent and grave complication among hematological patients, whose prevailing culprits are Carbapenem-Resistant Klebsiella pneumoniae (CRKP) and Escherichia coli bacteremia (EC). Nevertheless, there is a paucity of studies that have undertaken a comparative analysis of clinical outcomes in patients afflicted with CRKP and EC.
This study was conducted with the aim of identifying the microbiological and clinical characteristics of hematological patients suffering from bacteremia caused by CRKP and CREC.
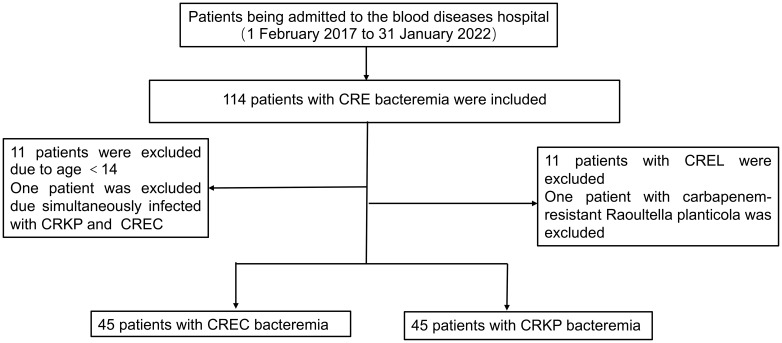
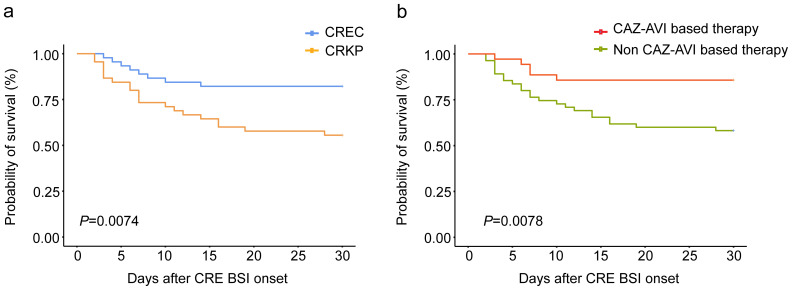
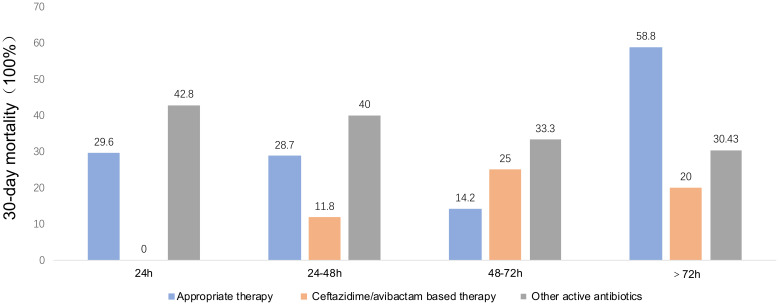
The cohort included 90 patients with equal proportions of CRKP BSI and CREC BSI from 2017 to 2022. Among the tested CRE strains (n = 45) for carbapenemase (CP) genes, the KPC gene was most commonly found in CP-CRKP isolates (12/21), while the NDM gene predominated among CP-CREC strains (18/24). A comparison of drug susceptibility showed that CREC was significantly more susceptible to tigecycline than CRKP (97.73% vs. 64.86%, P = 0.018). Patients treated with tigecycline-based therapy had a higher survival rate in the CREC group (18/24,75%) compared to the CRKP group (8/14,57.1%). The CRKP group had a significantly lower rate of prior cephalosporin use within 30 days compared to the CREC group (27% vs. 49%, P = 0.03) and a higher incidence of multi-site infections before BSI (44% vs. 8.9%, P<0.001). Multivariate analysis showed that BSI caused by CRKP was an independent risk factor for survival (P = 0.029), while CAZ-AVI-based therapy emerged as an independent factor improving patient prognosis (P =0.013).
Our results found that bacteremia instigated by CRKP was associated with a less favorable prognosis when compared to cases induced by CREC. Moreover, treatment regimens incorporating CAZ-AVI have the potential to enhance the prognosis of patients grappling with CRE BSI.
耐碳青霉烯类肠杆菌科细菌(CRE)血流感染(BSI)是血液系统疾病患者常见且严重的并发症,主要致病菌为耐碳青霉烯类肺炎克雷伯菌(CRKP)和大肠埃希菌菌血症(EC)。然而,对CRKP和EC感染患者的临床结局进行比较分析的研究较少。
本研究旨在确定CRKP和CREC所致菌血症血液系统疾病患者的微生物学和临床特征。
该队列包括2017年至2022年期间90例CRKP BSI和CREC BSI比例相等的患者。在检测的碳青霉烯酶(CP)基因的CRE菌株(n = 45)中,KPC基因在CP-CRKP分离株中最常见(12/21),而NDM基因在CP-CREC菌株中占主导(18/24)。药敏比较显示,CREC对替加环素的敏感性显著高于CRKP(97.73%对64.86%,P = 0.018)。与CRKP组(8/14,57.1%)相比,接受替加环素治疗的CREC组患者生存率更高(18/24,75%)。与CREC组相比,CRKP组在30天内使用头孢菌素的比例显著更低(27%对49%,P = 0.03),且BSI前多部位感染的发生率更高(44%对8.9%,P<0.001)。多因素分析显示,CRKP所致BSI是生存的独立危险因素(P = 0.029),而基于头孢他啶-阿维巴坦的治疗是改善患者预后的独立因素(P = 0.013)。
我们的结果发现,与CREC所致菌血症相比,CRKP所致菌血症的预后较差。此外,包含头孢他啶-阿维巴坦的治疗方案有可能改善CRE BSI患者的预后。