Kwon Ye In Christopher, Keller Michael, Elhigzi Kareem, Adibi Iman, Jones Holly Caboti, Lai Alan, Park Andrew Min-Gi, Tchoukina Inna F, Shah Keyur B, Fitch Zachary, Nicolato Patricia, Chery Josue, Quader Mohammed, Kasirajan Vigneshwar, Hashmi Zubair A
Division of Cardiothoracic Surgery, Department of Surgery, Pauley Heart Center, Virginia Commonwealth University School of Medicine, Richmond, Virginia, USA.
Division of Cardiology, Department of Internal Medicine, Pauley Heart Center, Virginia Commonwealth University School of Medicine, Richmond, Virginia, USA.
Clin Transplant. 2025 Jul;39(7):e70222. doi: 10.1111/ctr.70222.
Primary graft dysfunction (PGD) represents a leading cause of mortality in patients undergoing donation after brain death (DBD) orthotopic heart transplantation (OHT), requiring timely escalation to mechanical circulatory support. There is a lack of nationwide data regarding PGD after donation after circulatory death (DCD). Here, we evaluated the incidence and short-term outcomes of PGD following DCD.
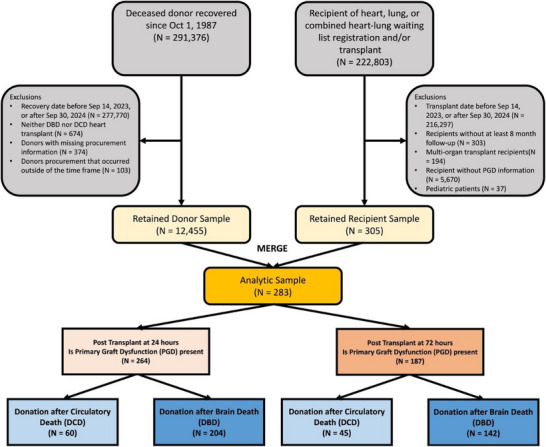
Using the UNOS registry between 9/2023 and 9/2024, we identified all adult (≥18 years) recipients of OHT. The incidence and outcomes of moderate-severe PGD (24- and 72-h post-transplant) were compared between DCD and DBD. Predictors for mortality after PGD were analyzed using Cox proportional hazard models. 30-day survival was analyzed using the Kaplan-Meier method.
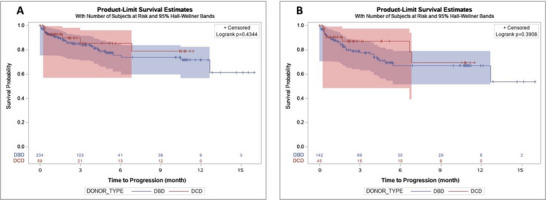
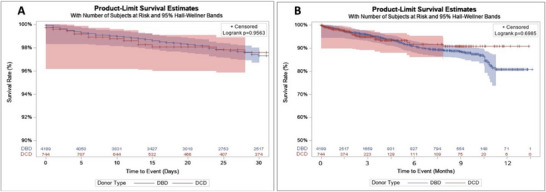
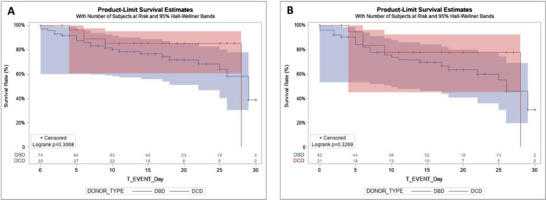
A total of 5017 patients underwent first-time OHT, among whom 762 (15.2%) received DCD hearts. DCD had a significantly higher incidence of PGD at 24- (7.9% vs. 4.8%; p = 0.001) and 72-h (5.9% vs. 3.3%; p = 0.001) compared to DBD. 30-day (p = 0.3068) survival was not different between DCD and DBD patients with PGD. Similarly, for recipients with PGD at 72 h, 30-day (p = 0.327) survival was comparable. At 72 h, DCD recipients were more likely to be supported on ECMO (p = 0.016). Transplanting DCD organs did not impact PGD-associated mortality at 24- (HR 0.72, p = 0.442) and 72-h (HR 0.74, p = 0.457). Postoperative ECMO was associated with decreased risk of PGD-associated mortality in DCD recipients at 24- (p < 0.0001) and 72-h (p < 0.0001).
While PGD rates appear higher in DCD, the associated mortality remains comparable to that of DBD. Early support on ECMO may confer survival benefits in DCD recipients with PGD.
原发性移植物功能障碍(PGD)是脑死亡后器官捐献(DBD)原位心脏移植(OHT)患者死亡的主要原因,需要及时升级到机械循环支持。目前缺乏关于循环死亡后器官捐献(DCD)后PGD的全国性数据。在此,我们评估了DCD后PGD的发生率和短期结局。
利用2023年9月至2024年9月的器官共享联合网络(UNOS)登记数据,我们确定了所有接受OHT的成年(≥18岁)受者。比较了DCD和DBD受者中重度PGD(移植后24小时和72小时)的发生率和结局。使用Cox比例风险模型分析PGD后死亡的预测因素。采用Kaplan-Meier方法分析30天生存率。
共有5017例患者接受了首次OHT,其中762例(15.2%)接受了DCD心脏。与DBD相比,DCD受者在24小时(7.9%对4.8%;p = 0.001)和72小时(5.9%对3.3%;p = 0.001)时PGD的发生率显著更高。发生PGD的DCD和DBD患者的30天生存率(p = 0.3068)无差异。同样,对于72小时发生PGD的受者,30天生存率(p = 0.327)相当。在72小时时,DCD受者更有可能接受体外膜肺氧合(ECMO)支持(p = 0.016)。移植DCD器官对24小时(风险比[HR] 0.72,p = 0.442)和72小时(HR 0.74,p = 0.457)时与PGD相关的死亡率没有影响。术后ECMO与DCD受者在24小时(p < 0.0001)和72小时(p < 0.0001)时与PGD相关的死亡风险降低相关。
虽然DCD中PGD的发生率似乎更高,但其相关死亡率与DBD相当。对发生PGD的DCD受者早期给予ECMO支持可能带来生存益处。