Elorza Garazi, Carré Miquel Kraft, Pellino Gianluca, de Andres Olabarria Unai, Marquina Teresa, Escovar Fernando Jiménez, Timoteo Ander, Gonzalez Jose Maria Garcia, Planellas Pere, Espín-Basany Eloy, Enriquez-Navascues Jose Maria
Colorectal Surgery, Hospital Universitario Donostia, Donostia, Spain.
Colorectal Surgery, Hospital Universitari Vall d´Hebron, Autonomous University of Barcelona, Barcelona, Spain.
Int J Colorectal Dis. 2025 Jul 8;40(1):153. doi: 10.1007/s00384-025-04939-1.
Primary objective was to compare the rates of parastomal hernia (PH) at 2 years after the creation of a terminal colostomy using two types of fascial incision: cross-shaped and reinforced longitudinal. Secondary objectives included the evaluation of postoperative complications, readmissions, reoperations for PH, and patients' quality of life.
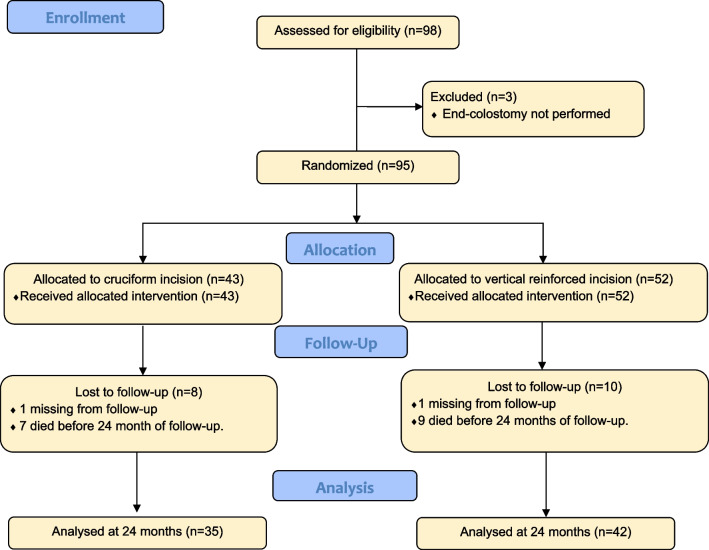
This was a multicenter superiority clinical trial conducted at 5 hospitals involving patients with rectal cancer and definitive colostomy. Patients were randomized into two groups: cross incision (n = 42) or reinforced longitudinal incision (n = 52), for the exteriorization of the colon in terminal colostomy. PH at 2 years was determined by physical examination, computed tomography (CT), and symptoms. Baseline data on risk factors for PH, postoperative complications, readmissions, reoperations for symptomatic PH, and quality of life were recorded.
A total of 95 patients were included: cross (n = 42) and reinforced longitudinal (n = 52). Demographic characteristics, risk factors for PH, and surgical factors were similar between the two groups. No significant differences were found in the clinical PH rate between the cruciate versus longitudinal incision groups (48.60% vs. 45.20%; p = 0.770), radiological PH (54.30% vs. 53.70%; p = 0.956), or symptomatic PH (14.30% vs. 19%; p = 0.579). The comprehensive complication index (CCI), readmissions, and reoperation rates for symptomatic PH (8.6% vs. 7.1%; p = 0.816) were similar in both groups. No significant differences were observed in the three health aspects evaluated using the EORTC QLQ-C30 scale.
The reinforcement of a longitudinal fascial incision as an isolated surgical technique does not reduce the incidence of PH after a 2-year follow-up.
主要目标是比较采用两种类型的筋膜切口(十字形和加强纵向切口)进行终末结肠造口术后2年的造口旁疝(PH)发生率。次要目标包括评估术后并发症、再入院情况、因PH进行的再次手术以及患者的生活质量。
这是一项在5家医院进行的多中心优效性临床试验,涉及直肠癌和确定性结肠造口术患者。患者被随机分为两组:十字形切口组(n = 42)或加强纵向切口组(n = 52),用于终末结肠造口术中结肠的外置。通过体格检查、计算机断层扫描(CT)和症状确定2年时的PH情况。记录PH危险因素、术后并发症、再入院情况、有症状PH的再次手术以及生活质量的基线数据。
共纳入95例患者:十字形切口组(n = 42)和加强纵向切口组(n = 52)。两组之间的人口统计学特征、PH危险因素和手术因素相似。十字形切口组与纵向切口组在临床PH发生率(48.60%对45.20%;p = 0.770)、放射学PH发生率(54.30%对53.70%;p = 0.956)或有症状PH发生率(14.30%对19%;p = 0.579)方面均未发现显著差异。两组的综合并发症指数(CCI)、再入院率和有症状PH的再次手术率(8.6%对7.1%;p = 0.816)相似。使用欧洲癌症研究与治疗组织QLQ-C30量表评估的三个健康方面未观察到显著差异。
作为一种单独的手术技术,加强纵向筋膜切口在2年随访后并未降低PH的发生率。