Kimura Kei, Takiyama Hirotoshi, Yamada Shigeru, Ito Kazuma, Koba Mizuki, Imada Ayako, Song Jihyung, Kataoka Kozo, Kihara Takako, Matsuda Ikuo, Beppu Naohito, Horio Yuki, Kitajima Kazuhiro, Uchino Motoi, Ikeuchi Hiroki, Ikeda Masataka
Division of Lower G.I., Department of Gastroenterological Surgery, School of Medicine, Hyogo Medical University, Nishinomiya 663-8501, Japan.
QST Hospital, National Institutes for Quantum Science and Technology, Chiba 263-8555, Japan.
Cancers (Basel). 2025 Jul 3;17(13):2230. doi: 10.3390/cancers17132230.
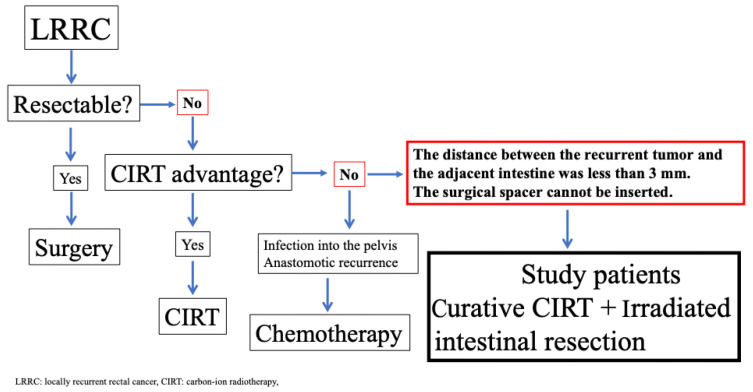
Carbon-ion radiotherapy (CIRT) is a promising treatment option for unresectable locally recurrent rectal cancer (LRRC). However, CIRT is contraindicated in cases where recurrent tumors are attached to the intestine. To address this limitation, we developed a novel treatment strategy involving curative-dose CIRT to recurrent tumors, including the adjacent intestine, without dose constraints, followed by surgical resection of the irradiated intestine. This study aimed to assess the feasibility of this approach. Patients were eligible for this study if the distance between the unresectable recurrent tumor and the adjacent intestines was less than 3 mm. Between 2019 and 2023, twelve patients were enrolled. CIRT was administered at curative doses of 70.4 or 73.6 Gy (relative biologic effectiveness (RBE)), including the adjacent intestines, without dose constraints. Surgical resection was not intended to excise the tumor itself, but was performed solely to remove the irradiated intestines. Irradiated intestine resection was planned within eight weeks after the completion of CIRT. All patients completed the scheduled treatment course. The median interval between completing CIRT and surgery was 4 (3-8) weeks. No patients experienced acute AEs related to CIRT. Regarding late AEs, two patients developed Grade I sciatic neuralgia, and one patient developed Grade III neuralgia. We considered this symptom, which later resulted in a limp in his left leg, acceptable because this patient could ambulate with assistance. Clavien-Dindo Grade III postoperative complications occurred in one patient. The median follow-up duration was 40 (20-60) months. One patient was diagnosed with in-field recurrence, and three patients were diagnosed with out-of-field recurrence. These patients received reirradiation with CIRT. Four patients experienced lung recurrence, and one patient died from rectal-cancer-specific causes. This novel treatment strategy may provide favorable outcomes for patients with unresectable LRRC. This approach can be applied to the currently accepted indications for CIRT, and we believe that CIRT is a feasible treatment option for future patients.
碳离子放疗(CIRT)是不可切除的局部复发性直肠癌(LRRC)一种很有前景的治疗选择。然而,当复发性肿瘤附着于肠道时,CIRT是禁忌的。为了解决这一局限性,我们制定了一种新的治疗策略,即对复发性肿瘤(包括相邻肠道)进行根治性剂量的CIRT,不受剂量限制,然后对受照射的肠道进行手术切除。本研究旨在评估这种方法的可行性。如果不可切除的复发性肿瘤与相邻肠道之间的距离小于3mm,则患者符合本研究的条件。在2019年至2023年期间,共有12名患者入组。以70.4或73.6Gy(相对生物效应(RBE))的根治性剂量进行CIRT,包括相邻肠道,不受剂量限制。手术切除并非旨在切除肿瘤本身,而仅仅是为了切除受照射的肠道。计划在CIRT完成后的八周内进行受照射肠道切除术。所有患者均完成了预定的治疗疗程。完成CIRT与手术之间的中位间隔时间为4(3 - 8)周。没有患者出现与CIRT相关的急性不良反应。关于迟发性不良反应,两名患者出现I级坐骨神经痛,一名患者出现III级神经痛。我们认为这种症状(该患者后来左腿跛行)是可以接受的,因为该患者在辅助下可以行走。一名患者发生了Clavien - Dindo III级术后并发症。中位随访时间为40(20 - 60)个月。一名患者被诊断为野内复发,三名患者被诊断为野外复发。这些患者接受了CIRT再照射。四名患者出现肺部复发,一名患者死于直肠癌特异性原因。这种新的治疗策略可能为不可切除的LRRC患者提供良好的治疗效果。这种方法可以应用于目前公认的CIRT适应证,我们相信CIRT对未来的患者是一种可行的治疗选择。