Pan Liwei, Lu Fengfeng, Cheng Bihuan, Zhang Wenwu, Wang Benji
Department of Anesthesiology, Critical Care and Pain Medicine, The Second Affiliated Hospital and Yuying Children's Hospital of Wenzhou Medical University, Wenzhou, 325000, Zhejiang, China.
J Health Popul Nutr. 2025 Jul 12;44(1):249. doi: 10.1186/s41043-025-01008-9.
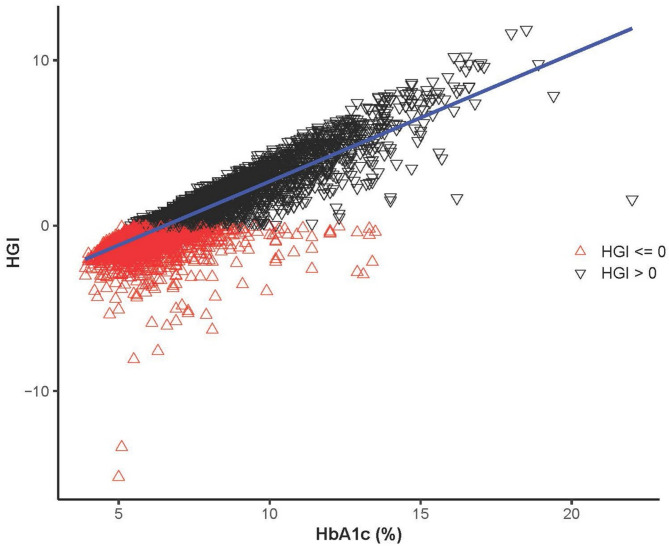
Glycemic variability is increasingly recognized as a critical factor influencing outcomes in intensive care, yet its prognostic role remains unclear. The Hemoglobin Glycation Index (HGI), which reflects individual glycemic variation, has not been thoroughly studied in critically ill populations.
To evaluate the association between HGI and all-cause mortality in critically ill patients using data from a large intensive care unit (ICU) cohort.
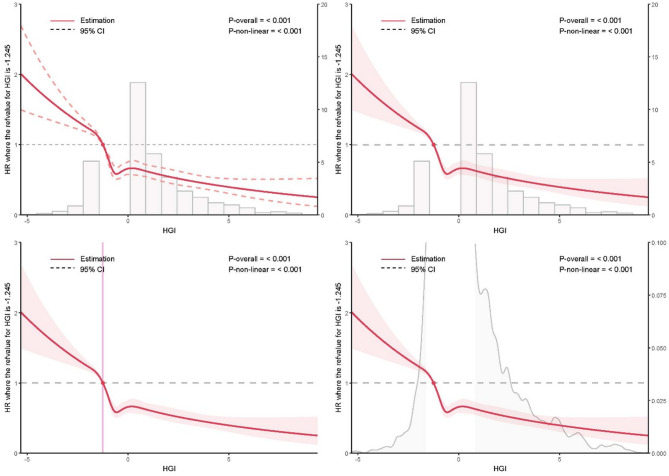
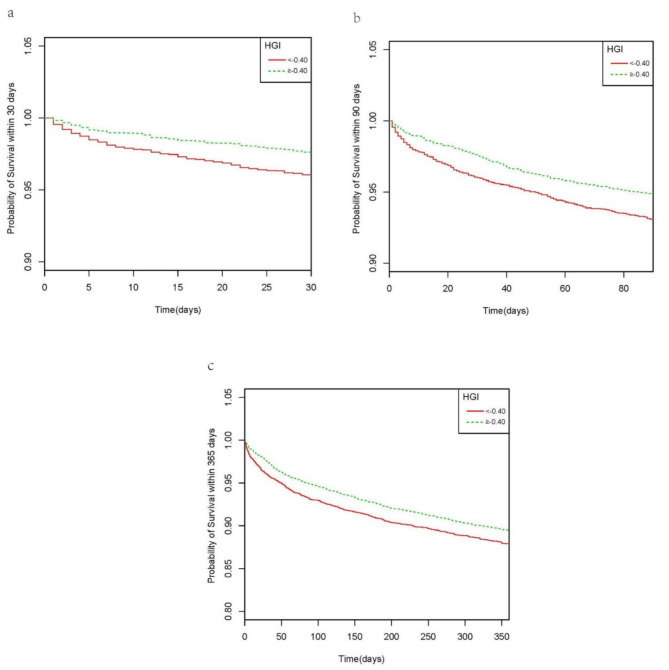
We conducted a retrospective cohort study using the MIMIC-IV database. The primary outcomes were 30-, 90-, and 365-day all-cause mortality; in-hospital mortality was secondary. Kaplan-Meier analysis, Cox regression, and restricted cubic spline (RCS) modeling were used to assess mortality risk across HGI levels. Propensity score matching (PSM) and subgroup analyses were performed to ensure robustness.
Among 9,695 patients, those with low HGI (< - 0.40) had significantly higher mortality (P < 0.001). RCS analysis showed a nonlinear association between HGI and 30-day mortality. Higher HGI values were independently associated with reduced risk of death at all time points, with hazard ratios ranging from 0.43 to 0.76 (P < 0.001). These associations persisted after multivariable adjustment and PSM. Subgroup analyses showed consistent results across patient characteristics.
Lower HGI values are associated with increased short- and long-term mortality in critically ill patients. HGI may serve as a valuable prognostic biomarker for risk stratification in ICU settings.
血糖变异性日益被认为是影响重症监护结局的关键因素,但其预后作用仍不明确。反映个体血糖变化的糖化血红蛋白指数(HGI)在危重症人群中尚未得到充分研究。
利用大型重症监护病房(ICU)队列的数据,评估危重症患者中HGI与全因死亡率之间的关联。
我们使用MIMIC-IV数据库进行了一项回顾性队列研究。主要结局为30天、90天和365天全因死亡率;院内死亡率为次要结局。采用Kaplan-Meier分析、Cox回归和限制性立方样条(RCS)建模来评估不同HGI水平下的死亡风险。进行倾向评分匹配(PSM)和亚组分析以确保结果的稳健性。
在9695例患者中,HGI低(< -0.40)的患者死亡率显著更高(P < 0.001)。RCS分析显示HGI与30天死亡率之间存在非线性关联。较高的HGI值在所有时间点均与死亡风险降低独立相关,风险比范围为0.43至0.76(P < 0.001)。这些关联在多变量调整和PSM后仍然存在。亚组分析显示不同患者特征的结果一致。
较低的HGI值与危重症患者短期和长期死亡率增加相关。HGI可能作为ICU环境中风险分层的有价值的预后生物标志物。