Kikuchi Ryosuke, Sasaki Kazuhito, Sato Yusuke, Niimi Aya, Sakamoto Akira, Nozawa Hiroaki, Murono Koji, Emoto Shigenobu, Yokoyama Yuichiro, Kaneko Kensuke, Kume Haruki, Ishihara Soichiro
Department of Surgical Oncology, Faculty of Medicine, The University of Tokyo, Tokyo, Japan.
Department of Urology, Faculty of Medicine, The University of Tokyo, Tokyo, Japan.
Int J Colorectal Dis. 2025 Jul 14;40(1):158. doi: 10.1007/s00384-025-04955-1.
Urinary dysfunction (UD) is still a major complication after lower rectal cancer (LRC) surgery. Untreated UD is an independent risk factor for renal dysfunction due to repeated urinary reflux and urinary tract infections. However, the relationship between postoperative UD and renal function following LRC surgery remains unclear. In this study, we investigated the impact of UD on renal function post-surgery.
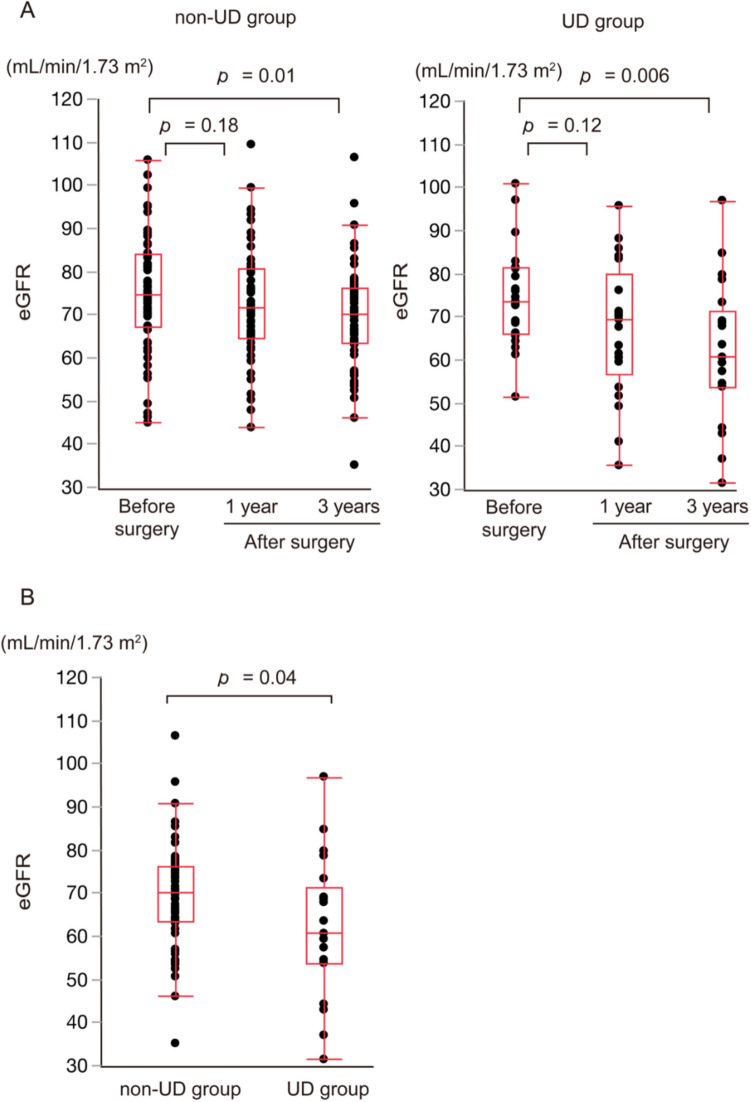
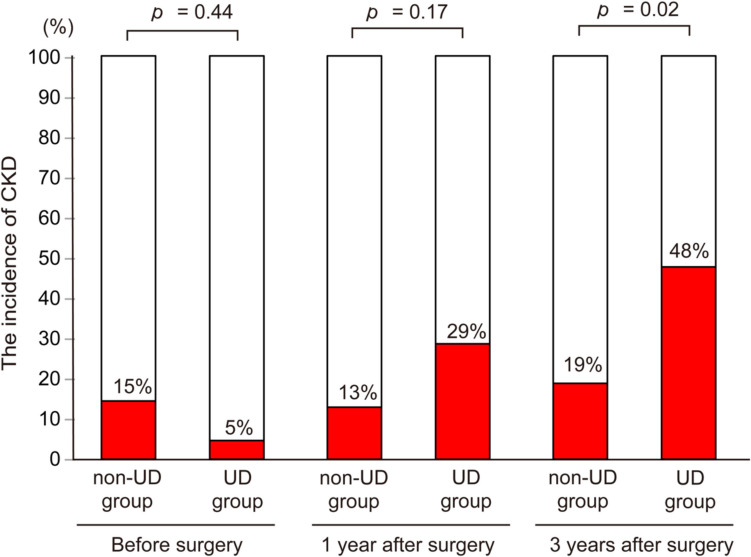
We retrospectively evaluated 83 patients with LRC who underwent curative resection at our tertiary referral center between April 2015 and December 2018. UD was diagnosed as a post-void residual urine volume ≥ 50 mL using uroflowmetry tests after discharge. We compared the estimated glomerular filtration rate (eGFR) and the incidence of chronic kidney disease (CKD)-defined as an eGFR < 60 mL/min/1.73 m-at 3 years after LRC surgery between the UD and non-UD groups. Patient selection was based on the criteria that excluded those with a history of urogenital interventions or incomplete postoperative follow-up. Statistical analysis used the Mann-Whitney U test for continuous variables, Fisher's test for categorical data, and multivariate logistic regression to adjust for potential confounders.
Of the 83 patients, 21 (25%) had UD. Patients with UD were older, underwent more extensive surgery, and had significantly longer operation times than those without UD. Within 3 years post-surgery, the UD group experienced a higher incidence of urinary tract complications and CKD, with a notable decrease in eGFR. Additionally, a history of hypertension and UD were identified as independent risk factors for CKD at 3 years post-surgery.
Patients with UD showed a significant decrease in eGFR and were more likely to progress to CKD at 3 years after LRC surgery. These findings indicated that postoperative UD might adversely affect renal function in patients with LRC.
排尿功能障碍(UD)仍是低位直肠癌(LRC)手术后的主要并发症。未经治疗的UD是因反复尿液反流和尿路感染导致肾功能障碍的独立危险因素。然而,LRC手术后术后UD与肾功能之间的关系仍不清楚。在本研究中,我们调查了UD对术后肾功能的影响。
我们回顾性评估了2015年4月至2018年12月期间在我们的三级转诊中心接受根治性切除的83例LRC患者。出院后通过尿流率测试将UD诊断为排尿后残余尿量≥50 mL。我们比较了UD组和非UD组在LRC手术后3年时的估计肾小球滤过率(eGFR)以及慢性肾脏病(CKD)的发生率,CKD定义为eGFR<60 mL/min/1.73 m²。患者选择基于排除有泌尿生殖系统干预史或术后随访不完整患者的标准。统计分析对连续变量使用曼-惠特尼U检验,对分类数据使用费舍尔检验,并使用多因素逻辑回归来调整潜在混杂因素。
83例患者中,21例(25%)有UD。与无UD的患者相比,有UD的患者年龄更大,接受的手术范围更广,手术时间明显更长。在术后3年内,UD组尿路并发症和CKD的发生率更高,eGFR显著下降。此外,高血压病史和UD被确定为术后3年时CKD的独立危险因素。
有UD的患者在LRC手术后3年时eGFR显著下降,且更有可能进展为CKD。这些发现表明术后UD可能对LRC患者的肾功能产生不利影响。