Daprà V, Gandini A, Schietroma F, Rossini D, Boccaccino A, Caira G, Calegari M A, Zoratto F, Costantini M, Formica V, Rofei M, Mauri G, Bonazzina E, Siena S, Iaia M L, Signorelli C, Antonuzzo L, Tamberi S, Foppa C, Spinelli A, Tortora G, Santoro A, Taieb J, Puccini A, Salvatore L
Department of Biomedical Sciences, Humanitas University, Pieve Emanuele, Milan, Italy; IRCCS Humanitas Research Hospital, Medical Oncology and Hematology Unit, Humanitas Cancer Center, Rozzano, Milan, Italy. Electronic address: https://twitter.com/ValeDapz.
Medical Oncology Unit 1, IRCCS Ospedale Policlinico San Martino, Genoa, Italy; Department of Gastroenterology and Gastrointestinal Oncology, CARPEM Comprehensive Cancer Center, Georges-Pompidou European Hospital, AP-HP, Paris, Université Paris-Cité, SIRIC CARPEM, Paris, France. Electronic address: https://twitter.com/AnnaliceGandini.
ESMO Open. 2025 Jul 15;10(8):105496. doi: 10.1016/j.esmoop.2025.105496.
T4 is one of the most important prognostic factors in localized colon cancer (CC), especially in stage II (pT4N0). However, the optimal adjuvant treatment in this subset of patients remains unclear. We present a large, multicenter, international, real-world analysis of pT4N0 CC patients.
A real-world database regarding clinicopathological characteristics of patients with stage II pT4N0 CC surgically removed between 2010 and 2021 was queried. Primary endpoints were overall survival (OS) and relapse-free survival (RFS), and analyses were adjusted on age (with a cut-off of 75 years) to reduce selection bias.
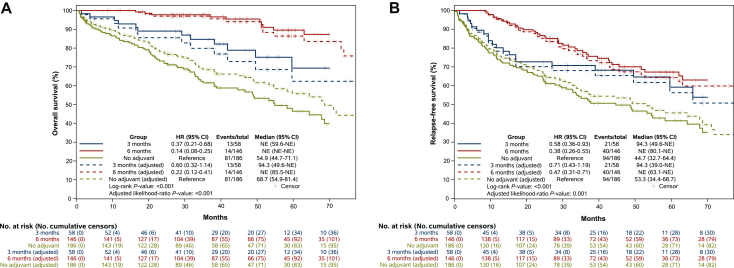
Our study included 492 patients; outcomes data were available for 390 patients. Median age was 73 years. Microsatellite status was assessed in 294 (75%), including 74 (25%) mismatch repair deficient (dMMR)/microsatellite instability (MSI). Adjuvant chemotherapy was prescribed in 204 patients (52%), mostly oxaliplatin-based (70%). After a median follow-up of 46.8 months, 6 months of adjuvant chemotherapy was associated with a significant improvement in OS [hazard ratio (HR) age-adjusted 0.22, P < 0.001] when compared with no adjuvant. The benefit was seen also with 3 months of adjuvant chemotherapy, even if the benefit was lower (HR age-adjusted 0.60, P < 0.001). Similar results were observed in terms of RFS, with a statistically significant benefit both in the 6-month group (HR age-adjusted 0.47, P = 0.001) and in the 3-month group (HR age-adjusted 0.71, P = 0.001). Considering the regimen and the duration of treatment, 6 months of oxaliplatin-based chemotherapy was associated with a significant improvement in both OS and RFS (P < 0.001). In univariate analysis, MMR status was not associated with OS nor RFS.
T4 was confirmed to be a poor prognostic factor. Adjuvant chemotherapy provided a large benefit, with a significant reduction in risk of recurrence and death. The benefit was proportional to its duration, and oxaliplatin-based chemotherapy may be better than monotherapy.
T4是局部结肠癌(CC)最重要的预后因素之一,尤其是在II期(pT4N0)。然而,这一亚组患者的最佳辅助治疗仍不明确。我们对pT4N0 CC患者进行了一项大型、多中心、国际性的真实世界分析。
查询了一个关于2010年至2021年期间手术切除的II期pT4N0 CC患者临床病理特征的真实世界数据库。主要终点为总生存期(OS)和无复发生存期(RFS),并根据年龄(以75岁为界)进行分析调整以减少选择偏倚。
我们的研究纳入了492例患者;390例患者有结局数据。中位年龄为73岁。对294例(75%)患者评估了微卫星状态,其中74例(25%)为错配修复缺陷(dMMR)/微卫星不稳定(MSI)。204例患者(52%)接受了辅助化疗,大多数是以奥沙利铂为基础的方案(70%)。中位随访46.8个月后,与未接受辅助化疗相比,6个月的辅助化疗与OS显著改善相关[年龄调整后的风险比(HR)为0.22,P < 0.001]。3个月的辅助化疗也有获益,尽管获益程度较低(年龄调整后的HR为0.60,P < 0.001)。在RFS方面观察到类似结果,6个月组(年龄调整后的HR为0.47,P = 0.001)和3个月组(年龄调整后的HR为0.71,P = 0.001)均有统计学显著获益。考虑治疗方案和持续时间,6个月的以奥沙利铂为基础的化疗与OS和RFS均显著改善相关(P < 0.001)。在单因素分析中,MMR状态与OS和RFS均无关。
T4被证实是一个不良预后因素。辅助化疗带来了显著益处,复发和死亡风险显著降低。获益与化疗持续时间成正比,以奥沙利铂为基础的化疗可能优于单一疗法。