Wong Esther, Chen Yiming, Kong Gwyneth, Chia Jobelle, Zhang Audrey, Mehta Anurag, Jayabaskaran Jayanth, Chong Bryan, Cao Grace, Nah Benjamin, Chan Mark Yan-Yee, Muthiah Mark, Loh Poay-Huan, Mamas Mamas A, Chew Nicholas Ws
Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore.
Department of Medicine, National University Hospital, Singapore, Singapore.
Sci Rep. 2025 Jul 21;15(1):26499. doi: 10.1038/s41598-025-12583-6.
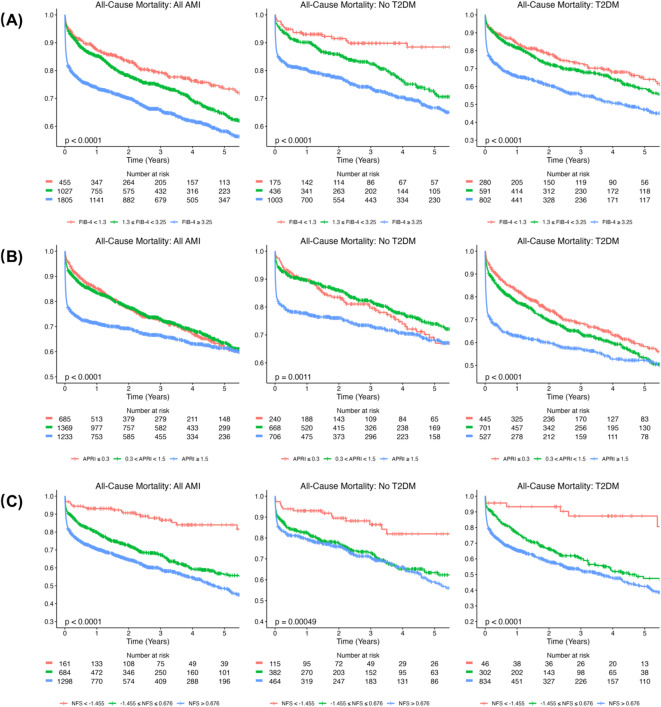
Patients with liver fibrosis and type 2 diabetes mellitus (T2DM) have an increased risk of cardiovascular events. However, long-term prognosis of liver fibrosis and T2DM after acute myocardial infarction (AMI) remain to be investigated. This study compared clinical characteristics and prognosis of AMI patients with T2DM and evidence of liver fibrosis. Patients were stratified into low, intermediate and high-risk for fibrosis, using serum-based non-invasive tests (NITs): Fibrosis-4 Index (FIB-4), Aspartate Aminotransferase to Platelet Ratio Index (APRI) and Non-alcoholic Fatty Liver Disease Fibrosis Score (NFS). The primary outcome was all-cause mortality, Kaplan-Meier curves were constructed for 5-year all-cause mortality. Cox regression analysis was used to determine the independent predictors of mortality, adjusting for confounders. Out of 3287 AMI patients, 1547 were stratified as high-risk by any NIT (mean follow-up duration 2.7 ± 2.3 years). A dose-response relationship was found with increasing mortality risk for higher APRI and NFS scores. High-risk FIB-4 also predicted mortality significantly (adjusted HR [aHR] 1.791, 95% CI 1.436-2.235, p < 0.001). High-risk FIB-4 and APRI independently predicted mortality regardless of T2DM status, while NFS only predicted mortality in T2DM patients. Following AMI, individuals stratified by FIB-4, APRI, NFS as high-risk for liver fibrosis were associated with excess long-term mortality (aHR 1.780, 95% CI 1.442-2.196, p < 0.001). Hence, readily available NITs may be beneficial in risk prognostication of AMI patients.
肝纤维化合并2型糖尿病(T2DM)的患者发生心血管事件的风险增加。然而,急性心肌梗死(AMI)后肝纤维化和T2DM的长期预后仍有待研究。本研究比较了伴有T2DM且有肝纤维化证据的AMI患者的临床特征和预后。使用基于血清的非侵入性检测(NITs):纤维化-4指数(FIB-4)、天冬氨酸转氨酶与血小板比值指数(APRI)和非酒精性脂肪性肝病纤维化评分(NFS),将患者分为低、中、高纤维化风险组。主要结局为全因死亡率,构建5年全因死亡率的Kaplan-Meier曲线。采用Cox回归分析确定死亡率的独立预测因素,并对混杂因素进行校正。在3287例AMI患者中,1547例被任何一种NIT分层为高风险(平均随访时间2.7±2.3年)。发现随着APRI和NFS评分升高,死亡风险呈剂量反应关系。高风险FIB-4也显著预测死亡率(校正后风险比[aHR]1.791,95%可信区间1.436-2.235,p<0.001)。无论T2DM状态如何,高风险FIB-4和APRI均独立预测死亡率,而NFS仅在T2DM患者中预测死亡率。AMI后,被FIB-4、APRI、NFS分层为肝纤维化高风险的个体与长期死亡率过高相关(aHR 1.780,95%可信区间1.442-2.196,p<0.001)。因此,易于获得的NITs可能有助于AMI患者的风险预后评估。