Meletti Stefano, Burani Margherita, Ballerini Alice, Giovannini Giada, Micalizzi Elisa, Orlandi Niccolò, Taruffi Lisa, Biagioli Niccolò, Scolastico Simona, Madrassi Laura, Pugnaghi Matteo, Vaudano Anna Elisabetta
Department of Biomedical, Metabolic and Neural Sciences, University of Modena and Reggio Emilia, Italy.
Neurophysiology Unit and Epilepsy Centre, Neuroscience Department, University of Modena, Italy.
Neurology. 2025 Aug 26;105(4):e213856. doi: 10.1212/WNL.0000000000213856. Epub 2025 Jul 22.
Postconvulsive central apnea has emerged as a contributor to sudden unexplained death in epilepsy. The aim of this study was to evaluate the incidence and characteristics of postictal central apnea (PICA) in focal seizures. The secondary aim was to analyze morphometric features of the amygdala and other subcortical structures involved in autonomic control.
We prospectively enrolled consecutive patients admitted to the Epilepsy Monitoring Unit at Modena Academic Hospital (Italy) from April 2020 to December 2023. Inclusion criteria were as follows: (1) age older than 13 years; (2) at least 1 focal-onset seizure recorded during long-term video-EEG monitoring (LTVEM) with cardiorespiratory polygraphy. For each seizure, the presence of ictal central apnea (ICA) and/or PICA and its features were evaluated. Amygdala, hippocampus, thalamus, brainstem, and cerebellum volumetry were compared in patients with ICA/PICA with respect to healthy controls and patients with focal seizures without peri-ictal breathing disorders.
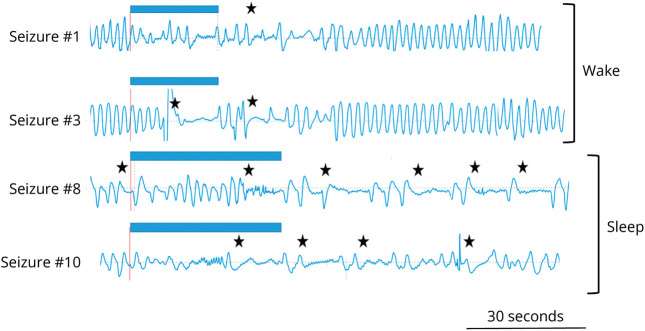
A total of 69 patients (mean age 35.7 years; 42% female) with 406 focal-onset seizures were analyzed. ICA was recorded in 71 seizures (17%) in 27 patients. PICA was recorded in 24 seizures in 12 patients (10 with temporal lobe epilepsy) corresponding to 5.9% of all recorded seizures. Notably, PICA was observed only in seizures showing ictal apnea (in 33.8%). In 11 seizures with PICA, a single apneic event starting in the ictal and extending to the postictal period was observed. In 13 seizures, multiple apneic events were present in the postictal period (range 2-8). Seizures with PICA showed a longer peri-ictal apnea time (mean 75 seconds vs 40 seconds; = 0.007) and a longer time to restore a regular rhythmic breathing after seizure termination (mean 173 seconds vs 42 seconds; < 0.001) than seizures with self-limiting ictal apnea. Amygdala volumes ipsilateral to the epileptogenic zone were larger in patients with ICA/PICA compared with controls and patients without seizure-related apnea.
PICA occurs in approximately 6% of focal seizures and is associated with extended apnea time and an enlarged amygdala ipsilaterally to the epileptogenic zone. Our data support the existence of a continuum from ictal to PICA and highlight the importance of cardiorespiratory recordings in LTVEM.
惊厥后中枢性呼吸暂停已成为癫痫不明原因猝死的一个因素。本研究的目的是评估局灶性癫痫发作后发作期中枢性呼吸暂停(PICA)的发生率和特征。次要目的是分析杏仁核和其他参与自主控制的皮质下结构的形态学特征。
我们前瞻性地纳入了2020年4月至2023年12月在意大利摩德纳大学医院癫痫监测病房连续入院的患者。纳入标准如下:(1)年龄大于13岁;(2)在长期视频脑电图监测(LTVEM)及心肺多导记录中至少记录到1次局灶性发作。对于每次发作,评估发作期中枢性呼吸暂停(ICA)和/或PICA的存在及其特征。将有ICA/PICA的患者的杏仁核、海马、丘脑、脑干和小脑体积与健康对照以及无发作期呼吸障碍的局灶性癫痫患者进行比较。
共分析了69例患者(平均年龄35.7岁;42%为女性)的406次局灶性发作。27例患者的71次发作(17%)记录到ICA。12例患者(10例为颞叶癫痫)的24次发作记录到PICA,占所有记录发作的5.9%。值得注意的是,仅在出现发作期呼吸暂停的发作中观察到PICA(占33.8%)。在11次有PICA的发作中,观察到单个呼吸暂停事件始于发作期并延伸至发作后期。在13次发作中,发作后期出现多次呼吸暂停事件(范围为2 - 8次)。与有自限性发作期呼吸暂停的发作相比,有PICA的发作显示发作期呼吸暂停时间更长(平均75秒对40秒;P = 0.007),发作终止后恢复有规律节律性呼吸的时间更长(平均173秒对42秒;P < 0.001)。与对照组和无发作相关呼吸暂停的患者相比,有ICA/PICA的患者癫痫发作灶同侧的杏仁核体积更大。
PICA发生在约6%的局灶性发作中,与延长的呼吸暂停时间和癫痫发作灶同侧杏仁核增大有关。我们的数据支持从发作期到PICA存在连续性,并强调了LTVEM中心肺记录的重要性。