Zhao Xiaofen, Le Yuanjie, Xin Ting, Gao Guosheng, Zhu Mengya, Xun Kai, Mao Xinliang
Department of Intensive Care Medicine, Ningbo No. 2 Hospital, Ningbo, China.
Department of Emergency Medicine, Ningbo No. 2 Hospital, Ningbo, China.
Front Neurol. 2025 Jul 8;16:1564063. doi: 10.3389/fneur.2025.1564063. eCollection 2025.
Hemorrhagic transformation (HT) is a critical complication of endovascular therapy (EVT) in acute ischemic stroke (AIS), significantly worsening patient outcomes. Although various risk factors have been identified, existing predictive models often fail to account for the multimodal nature of EVT and the complex interplay of clinical, imaging, and laboratory variables.
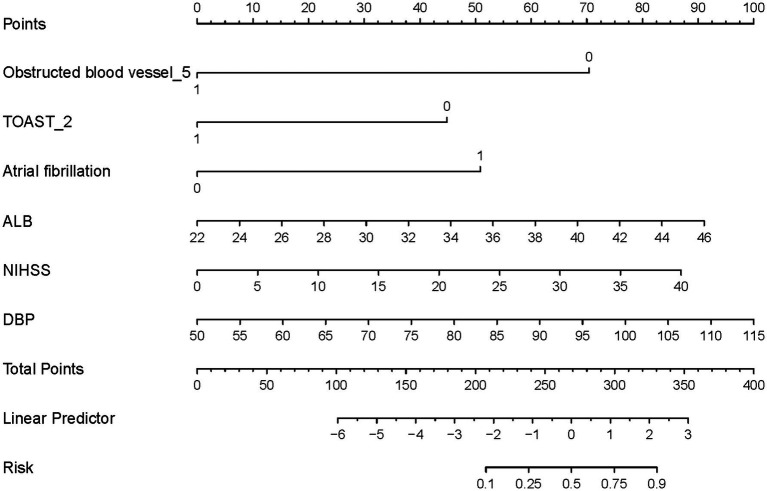
This study aimed to develop and validate a nomogram-based predictive model to estimate the risk of HT in AIS patients undergoing EVT, incorporating clinical, imaging, and laboratory data to provide a comprehensive risk assessment.
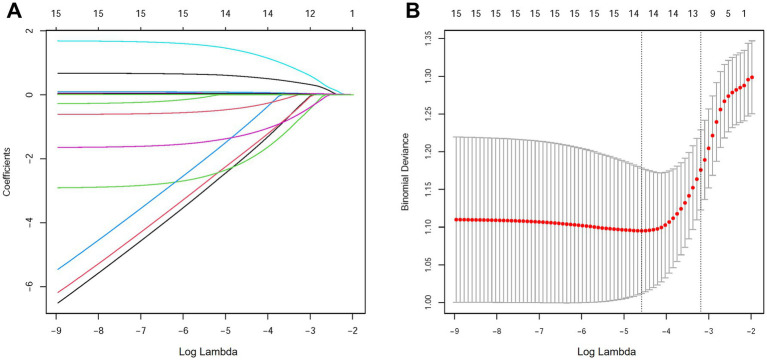
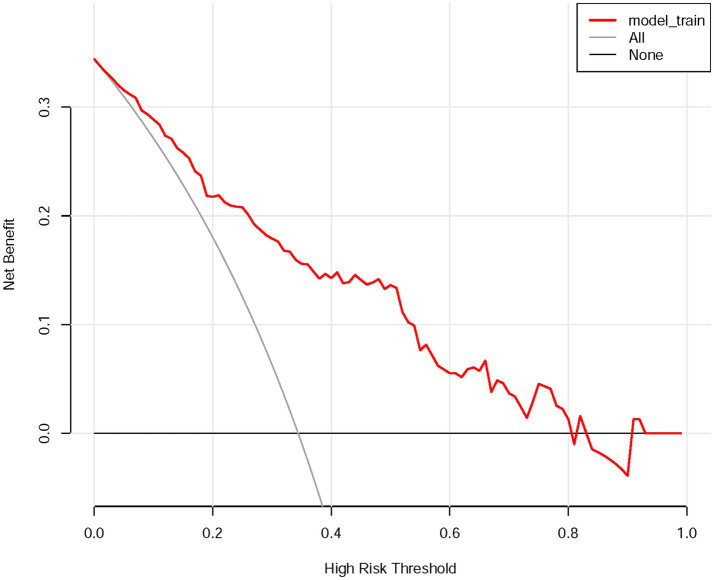
A retrospective analysis was performed on 154 AIS patients who underwent EVT at a single center between 2018 and 2023. The least absolute shrinkage and selection and operator (LASSO) and multivariate logistic regression were used to identify the independent predictors of HT. A nomogram was constructed and evaluated using the area under the receiver operating characteristic curve (AUC-ROC), calibration curves, and decision curve analysis (DCA).
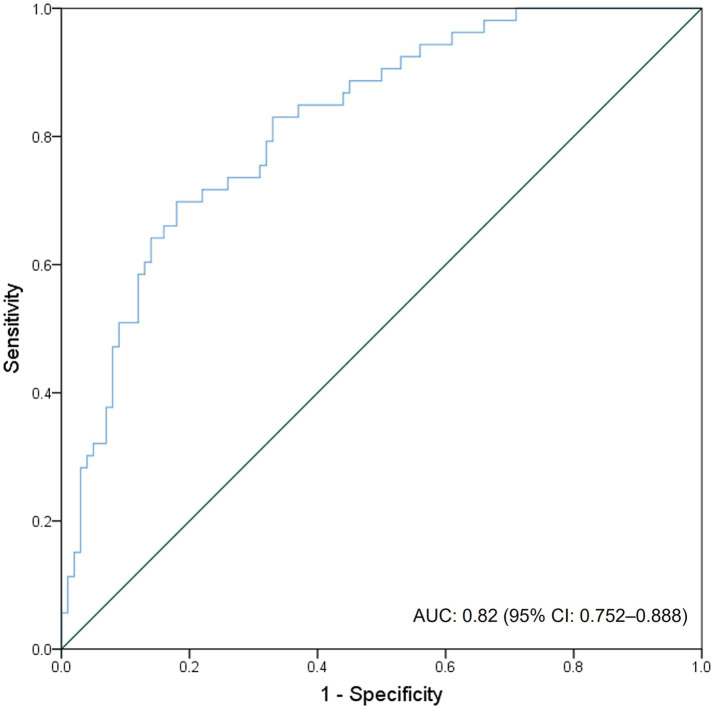
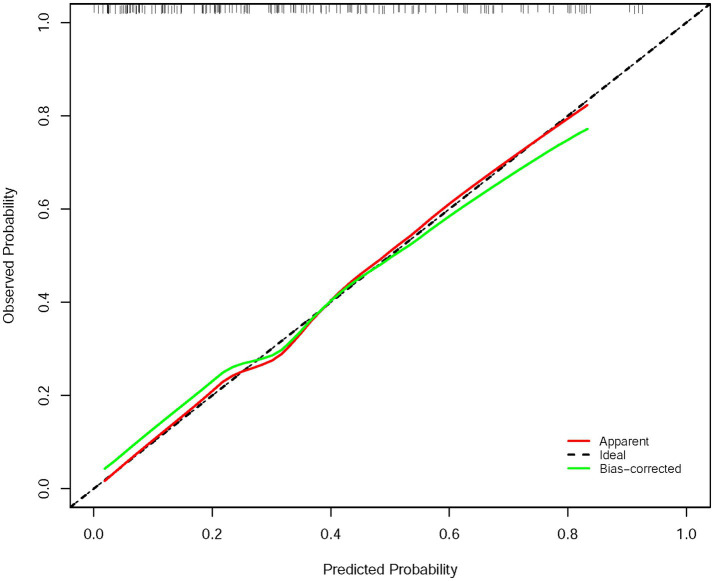
Among the 154 patients, 34.4% experienced HT. The nomogram demonstrated excellent discriminatory ability, with an AUC-ROC of 0.82 (95% CI: 0.752-0.888), and strong calibration, as indicated by calibration curves. DCA confirmed the model's clinical utility when the threshold probability was <0.8. Six independent prediction factors of HT were identified: atrial fibrillation (OR: 6.152), albumin (OR: 1.145), baseline NIHSS score (OR: 1.081), diastolic blood pressure (OR: 1.057), Trial of ORG 10172 in Acute Stroke Treatment (TOAST) Classification (TOAST_2, cardioembolic stroke subtype, OR: 0.201), and the location of obstructed blood vessel_5 (basilar artery occlusion, OR: 0.081).
The developed nomogram provides an accurate, individualized risk assessment of HT in AIS patients undergoing EVT. This tool enables personalized risk stratification, aiding clinicians in optimizing treatment strategies and improving patient outcomes. Further multicenter validation is warranted to generalize these findings.
出血性转化(HT)是急性缺血性卒中(AIS)血管内治疗(EVT)的一种关键并发症,会显著恶化患者预后。尽管已确定了多种危险因素,但现有的预测模型往往未能考虑到EVT的多模态性质以及临床、影像和实验室变量之间的复杂相互作用。
本研究旨在开发并验证一种基于列线图的预测模型,以估计接受EVT的AIS患者发生HT的风险,纳入临床、影像和实验室数据以提供全面的风险评估。
对2018年至2023年间在单一中心接受EVT的154例AIS患者进行回顾性分析。采用最小绝对收缩和选择算子(LASSO)和多因素逻辑回归来确定HT的独立预测因素。使用受试者操作特征曲线下面积(AUC-ROC)、校准曲线和决策曲线分析(DCA)构建并评估列线图。
154例患者中,34.4%发生了HT。列线图显示出优异的区分能力,AUC-ROC为0.82(95%CI:0.752-0.888),校准曲线表明校准效果良好。DCA证实当阈值概率<0.8时该模型具有临床实用性。确定了HT的六个独立预测因素:心房颤动(OR:6.152)、白蛋白(OR:1.145)、基线美国国立卫生研究院卒中量表(NIHSS)评分(OR:1.081)、舒张压(OR:1.057)、急性卒中治疗中ORG 10172试验(TOAST)分类(TOAST_2,心源性栓塞性卒中亚型,OR:0.201)以及阻塞血管的位置_5(基底动脉闭塞,OR:0.081)。
所开发的列线图为接受EVT的AIS患者提供了准确的、个体化的HT风险评估。该工具能够实现个性化风险分层,帮助临床医生优化治疗策略并改善患者预后。有必要进行进一步的多中心验证以推广这些发现。