Marroncelli Nunzio, Ambrosini Giulia, Errico Andrea, Vinco Sara, Dalla Pozza Elisa, Cogo Giulia, Cristanini Ilaria, Migliorini Filippo, Zampieri Nicola, Dando Ilaria
Department of Neurosciences, Biomedicine and Movement Sciences, University of Verona, 37134 Verona, Italy.
UOC of Urology, Azienda Ospedaliera Universitaria Integrata di Verona, 37126 Verona, Italy.
Cancers (Basel). 2025 Jul 21;17(14):2409. doi: 10.3390/cancers17142409.
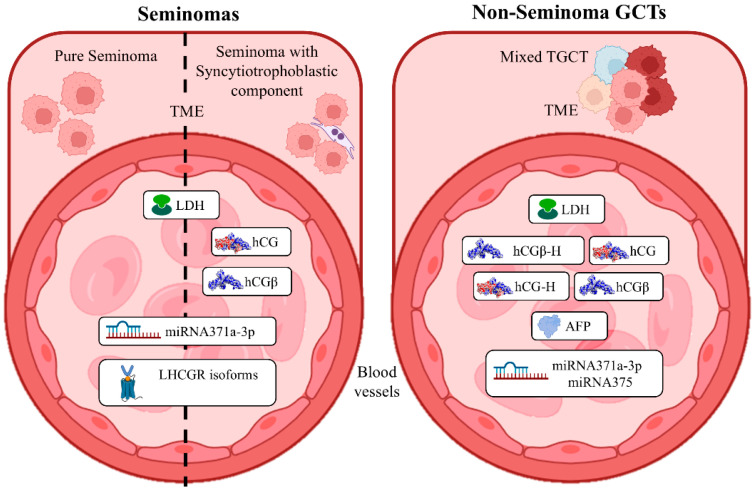
Testicular germ cell tumors (TGCTs) are the most common malignancies affecting young men between the ages of 14 and 44, accounting for about 95% of all testicular cancers. Despite being relatively rare compared to other cancers (~3.0 cases per 100,000 population, with high worldwide variability), TGCTs' incidence is increasing, particularly in industrialized countries. The initial phase of TGCT diagnosis is performed by detecting in the blood the presence of three proteins, i.e., alpha-fetoprotein (AFP), lactate dehydrogenase (LDH), and human chorionic gonadotropin (hCG). Despite these proteins being defined as markers of TGCTs, they present limitations in specificity. Indeed, AFP is not elevated in pure seminomas; LDH serum levels can be elevated in other conditions, such as liver disease or tissue damage, and hCG can be elevated in both seminomas and non-seminomas, reducing its ability to differentiate between tumor types. However, the existence of hCG variants, characterized by distinct glycosylation profiles that are differentially expressed in TGCT types and subtypes, may increase the diagnostic and prognostic potential of this hormone. Furthermore, emerging molecular biomarkers, including miRNAs and tumor cells-related epigenetic status, may offer new promising alternatives to improve diagnostic accuracy. Nonetheless, standardized diagnostic protocols still need to be implemented. Finally, understanding the biological roles of hCG isoforms and their "canonical" (e.g., LHCGR) and "non-canonical" (e.g., TGF-βR) receptor interactions may help in understanding tumor biology and therapeutic targeting.
睾丸生殖细胞肿瘤(TGCTs)是影响14至44岁年轻男性的最常见恶性肿瘤,约占所有睾丸癌的95%。尽管与其他癌症相比相对罕见(每10万人中约有3.0例,全球差异较大),但TGCTs的发病率正在上升,尤其是在工业化国家。TGCT诊断的初始阶段是通过检测血液中三种蛋白质的存在来进行的,即甲胎蛋白(AFP)、乳酸脱氢酶(LDH)和人绒毛膜促性腺激素(hCG)。尽管这些蛋白质被定义为TGCTs的标志物,但它们在特异性方面存在局限性。事实上,纯精原细胞瘤中AFP不升高;LDH血清水平在其他情况下可能升高,如肝病或组织损伤,而hCG在精原细胞瘤和非精原细胞瘤中均可升高,这降低了其区分肿瘤类型的能力。然而,hCG变体的存在,其特征在于在TGCT类型和亚型中差异表达的不同糖基化谱,可能会增加这种激素的诊断和预后潜力。此外,包括微小RNA和肿瘤细胞相关表观遗传状态在内的新兴分子生物标志物,可能为提高诊断准确性提供新的有前景的替代方法。尽管如此,仍需实施标准化的诊断方案。最后,了解hCG异构体的生物学作用及其“经典”(如LHCGR)和“非经典”(如TGF-βR)受体相互作用,可能有助于理解肿瘤生物学和治疗靶点。