Attahiru Adam, Mohammed Yahaya, Mikailu Fiyidi, Waziri Hyelshilni, Waziri Ndadilnasiya Endie, Tukur Mustapha, Sunusi Bashir, Mahmoud Mohammed Nasir, Vollmer Nancy, Vargas William, Yusufari Yusuf, Corrêa Gustavo, Reynolds Heidi W, Fisseha Teemar, Bello Talatu Buba, Kamateeka Moreen, Adewole Adefisoye Oluwaseun, Bello Musa, Bello Imam Wada, Etamesor Sulaiman, Valadez Joseph J, Nguku Patrick
African Field Epidemiology Network (AFENET), Abuja 900231, Nigeria.
Kano State Primary Health Care Development Agency, Kano 700101, Nigeria.
Vaccines (Basel). 2025 Jun 20;13(7):664. doi: 10.3390/vaccines13070664.
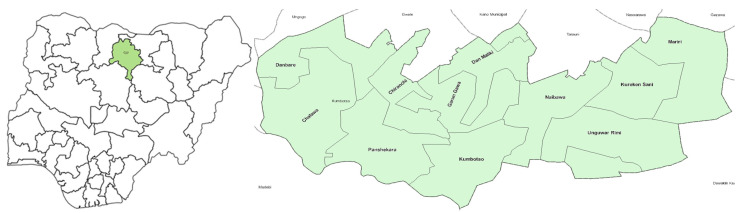
Immunization coverage in Nigeria is low, with many children missing out on important lifesaving vaccines. To enable a better understanding of contextual factors towards increasing uptake, we piloted a Decentralized Immunization Monitoring (DIM) approach in the Kumbotso local government area (LGA) of Kano state, Nigeria, to identify wards with low vaccination rates and understand why this is happening. The findings were used to improve routine immunization (RI) programs and reduce the number of unvaccinated children and children yet to receive their first dose of diphtheria-pertussis-tetanus (DPT) vaccine, referred to as Zero-Dose children (ZD).
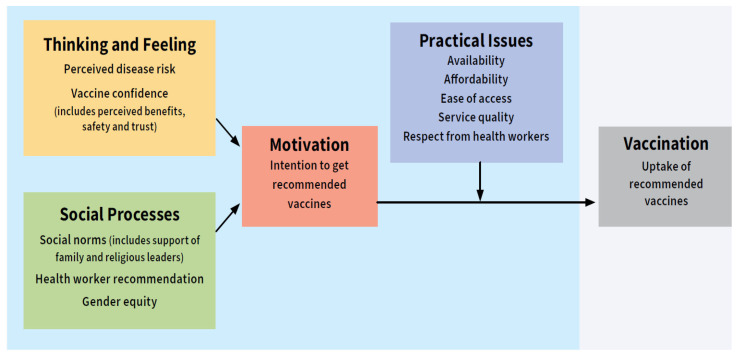
This study adopted a cross-sectional design approach using the Behavioural and Social Drivers of Vaccination (BeSD) framework and the Lot Quality Assurance Sampling (LQAS). The study population comprised caregivers of children aged 0-11 months and 12-23 months across the 11 wards in Kumbotso District, Kano State, Nigeria, using a segmentation sampling approach. The study covered 209 settlements selected using probability proportionate to size (PPS) sampling from the wards. Univariate and bivariate analyses were performed to show patterns and relations across variables.
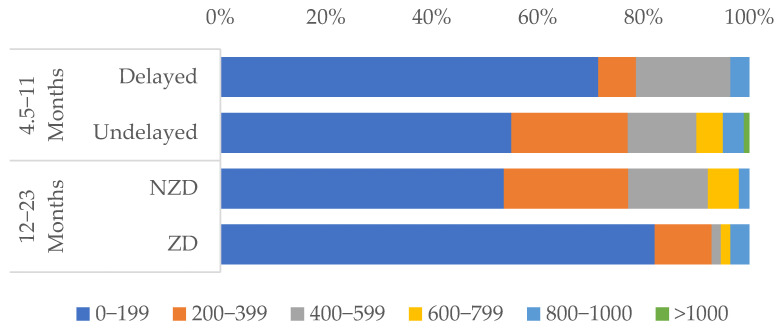
Out of 418 caregivers surveyed, 98.1% were female. Delayed vaccination was experienced by 21.9% of children aged 4.5-11 months, while the prevalence of ZD was estimated at 26.8% amongst the older cohort (12-23 months). A total of 71.4% of the delayed group and 89.1% of the ZD group remained unvaccinated. Caregiver education, rural residence, and home births correlated with delayed/ZD status ( < 0.05). Logistic regression associated higher caregiver education with reduced delayed vaccination odds (OR:0.34, < 0.001) and urban residence with lower ZD odds (OR:1.89, = 0.036). The antigen coverages of BCG (81.5%), DPT3 (63.6%), and measles 1 (59.7%) all surpassed the national dropout thresholds. Kumbotso, Unguwar Rimi, and Kureken Sani wards were all identified as underperforming and therefore targeted for intervention. Negative vaccine perceptions (50% delayed, 53.6% ZD) and distrust in health workers (46.4% delayed, 48.2% ZD) were significant barriers, though the caregiver intent to vaccinate was protective (OR: 0.27, < 0.001). The cost of accessing immunization services appeared to have a minor effect on coverage, as the majority of caregivers of delayed and ZD children reported spending less than 200 Naira (equivalent to USD 0.15) on transport.
This pilot study highlighted the utility of LQAS and BeSD in identifying low-performing wards, barriers, and routine immunization gaps. Barriers included low caregiver education, rural residence, and negative vaccine perceptions/safety. Caregiver education and urban residence were protective factors against delayed and ZD vaccination, suggesting social and systemic barriers, particularly in rural and less educated populations. Antigen-specific coverage showed disparities, with dropouts for multi-dose vaccines exceeding the national thresholds of 10%. Targeted measures addressing education, trust, and systemic issues are needed. Findings emphasize decentralized monitoring, community engagement, and context-specific strategies to reduce ZD children and ensure equitable vaccination in Nigeria.
尼日利亚的免疫接种覆盖率较低,许多儿童未能接种重要的救命疫苗。为了更好地了解影响疫苗接种率提高的背景因素,我们在尼日利亚卡诺州昆博索地方政府辖区(LGA)试点了一种分散式免疫监测(DIM)方法,以确定疫苗接种率较低的病房,并了解其原因。研究结果用于改进常规免疫(RI)计划,减少未接种疫苗儿童以及尚未接种第一剂白喉 - 百日咳 - 破伤风(DPT)疫苗的儿童(即零剂量儿童,ZD)的数量。
本研究采用横断面设计方法,使用疫苗接种的行为和社会驱动因素(BeSD)框架以及批量质量保证抽样(LQAS)。研究人群包括尼日利亚卡诺州昆博索区11个病房中0 - 11个月和12 - 23个月儿童的看护人,采用分层抽样方法。该研究涵盖了从病房中使用按规模比例概率抽样(PPS)选择的209个定居点。进行单变量和双变量分析以显示变量之间的模式和关系。
在接受调查的418名看护人中,98.1%为女性。4.5 - 11个月大的儿童中有21.9%经历了疫苗接种延迟,而在年龄较大的队列(12 - 23个月)中,ZD的患病率估计为26.8%。延迟接种组中共有71.4%的儿童以及ZD组中89.1%的儿童仍未接种疫苗。看护人的教育程度、农村居住情况和家庭分娩与延迟接种/ZD状态相关(<0.05)。逻辑回归表明,看护人教育程度较高与延迟接种几率降低相关(OR:0.34,<0.001),城市居住与ZD几率较低相关(OR:1.89,=0.036)。卡介苗(BCG)(81.5%)、三联疫苗(DPT3)(63.6%)和麻疹疫苗1(59.7%)的抗原覆盖率均超过了国家脱漏阈值。昆博索、翁古瓦尔·里米和库雷肯·萨尼病房均被确定为表现不佳,因此被列为干预目标。对疫苗持负面看法(延迟接种组中占50%,ZD组中占53.6%)和对卫生工作者不信任(延迟接种组中占46.4%,ZD组中占48.2%)是显著障碍,不过看护人的接种意愿具有保护作用(OR:0.27,<0.001)。获得免疫服务的成本似乎对覆盖率影响较小,因为延迟接种和ZD儿童的大多数看护人报告交通费用支出不到200奈拉(相当于0.15美元)。
这项试点研究突出了LQAS和BeSD在识别表现不佳的病房、障碍和常规免疫差距方面的作用。障碍包括看护人教育程度低、农村居住情况以及对疫苗的负面看法/安全性担忧。看护人教育程度和城市居住情况是预防延迟接种和ZD接种的保护因素,这表明存在社会和系统性障碍,特别是在农村和教育程度较低的人群中。抗原特异性覆盖率存在差异,多剂量疫苗的脱漏率超过了国家10%的阈值。需要采取针对性措施来解决教育、信任和系统性问题。研究结果强调了分散式监测、社区参与以及针对具体情况的策略,以减少ZD儿童数量并确保尼日利亚的公平疫苗接种。