Shao Cong, Wan Quan, Guo Jia, Chen Zhuo
Hebi Institute of Engineering and Technology, Henan Polytechnic University, Hebi, China.
Department of Urology, Xi'an Electric Power Central Hospital, Xi'an, China.
Front Pharmacol. 2025 Jul 17;16:1586650. doi: 10.3389/fphar.2025.1586650. eCollection 2025.
Cabazitaxel (CAB) has been approved for the treatment of patients with progressed metastatic castration-resistant prostate cancer (mCRPC) after receiving docetaxel. To assess the efficacy and safety of CAB in mCRPC patients through systematic review and network meta-analysis.
Randomized controlled studies on the treatment of mCRPC with CAB in PUBMED, EMBASE, Cochrane, and Web of Science were searched. Relevant studies that met pre-set criteria were determined, and the quality of included studies was evaluated using the National Institutes of Health-Quality Assessment Tool. After the data was extracted, data analysis was conducted in R 4.3.2. Overall survival (OS), progression-free survival (PFS), and serious adverse events (SAEs) were used as the primary outcomes, and HR (hazard ratio) or RR (risk ratio) and their 95% confidence intervals (95% CrI) were calculated as effect sizes.
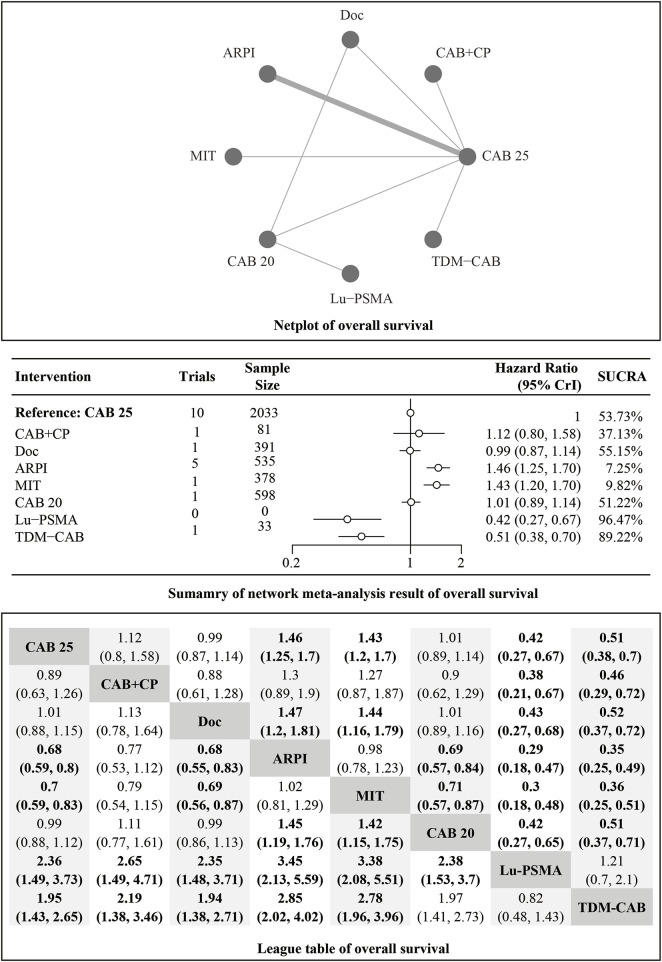
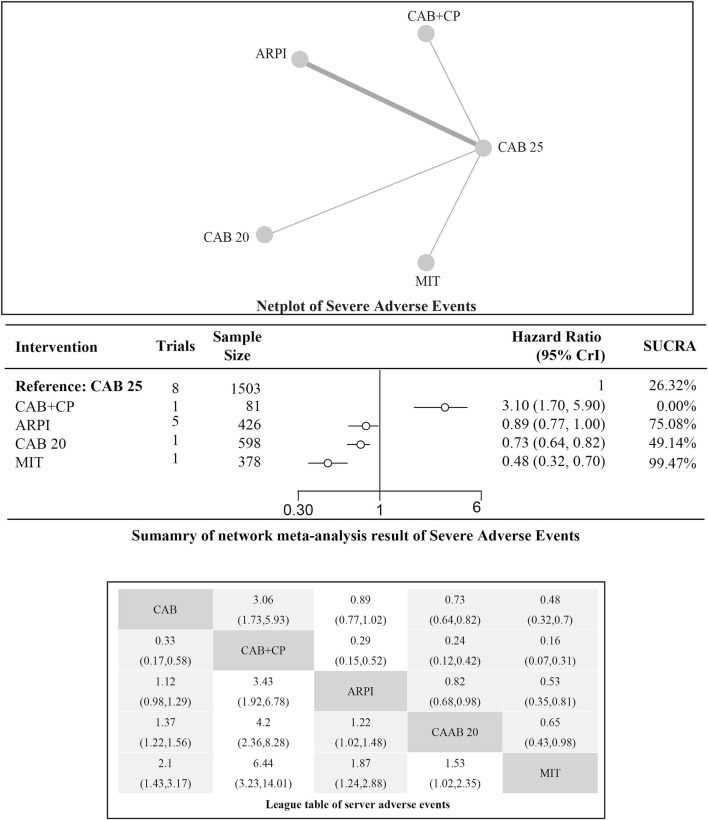
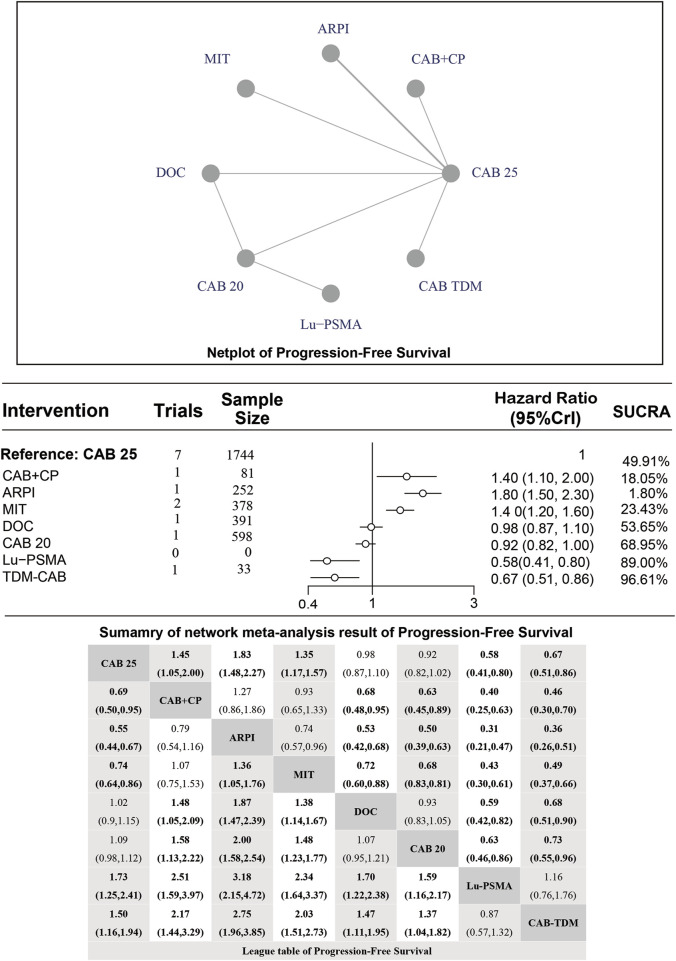
A total of 13 studies were included, involving 5,814 patients. The overall risk of bias for 13 studies was low. The results showed that CAB 25 mg/m significantly improved OS compared to androgen receptor pathway inhibitor (ARPI) (1.50 [1.30, 1.70]) and MIT (1.40 [1.20, 1.70]), but its efficacy was inferior to Lu-PSMA (0.42 [0.27, 0.67]) and therapeutic drug monitoring (TDM)-CAB (0.51 [0.38, 0.70]). CAB 25 mg/m could significantly improve PFS compared to CAB + CP (1.40 [1.10, 2.00]), ARPI (1.80 [1.50, 2.30], MIT (1.40 [1.20, 1.60]), but its efficacy was not as good as CAB 20 mg/m (0.92 [0.82, 1.00]), Lu-PSMA (0.58 [0.41, 0.80]), TDM-CAB (0.67 [0.51, 0.86]). In addition, compared to CAB 25 mg/m, CAB + CP may significantly increase the risk of SAEs (3.10 [1.70, 5.90]).
CAB is an effective treatment in mCRPC, and combining it with other treatment methods may enhance efficacy, but attention should be paid to the occurrence of adverse events.
卡巴他赛(CAB)已被批准用于治疗接受多西他赛后病情进展的转移性去势抵抗性前列腺癌(mCRPC)患者。通过系统评价和网状Meta分析评估CAB在mCRPC患者中的疗效和安全性。
检索PUBMED、EMBASE、Cochrane和Web of Science中关于CAB治疗mCRPC的随机对照研究。确定符合预设标准的相关研究,并使用美国国立卫生研究院质量评估工具评估纳入研究的质量。提取数据后,在R 4.3.2中进行数据分析。总生存期(OS)、无进展生存期(PFS)和严重不良事件(SAEs)作为主要结局指标,计算风险比(HR)或比值比(RR)及其95%可信区间(95% CrI)作为效应量。
共纳入13项研究,涉及5814例患者。13项研究的总体偏倚风险较低。结果显示,与雄激素受体通路抑制剂(ARPI)(1.50 [1.30, 1.70])和米托蒽醌(MIT)(1.40 [1.20, 1.70])相比,25mg/m²的CAB显著改善了OS,但其疗效不如镥[¹⁷⁷Lu]前列腺特异性膜抗原(Lu-PSMA)(0.42 [0.27, 0.67])和治疗药物监测(TDM)-CAB(0.51 [0.38, 0.70])。与CAB + 卡铂(CP)(1.40 [1.10, 2.00])、ARPI(1.80 [1.50, 2.30])、MIT(1.40 [1.20, 1.60])相比,25mg/m²的CAB可显著改善PFS,但其疗效不如20mg/m²的CAB(0.92 [0.82, 1.00])、Lu-PSMA(0.58 [0.41, 0.80])、TDM-CAB(0.67 [0.51, 0.86])。此外,与25mg/m²的CAB相比,CAB + CP可能显著增加SAEs的风险(3.10 [1.70, 5.90])。
CAB是治疗mCRPC的有效方法,与其他治疗方法联合使用可能提高疗效,但应注意不良事件的发生。