Endeshaw Amanuel Sisay, Kumie Fantahun Tarekegn, Debas Simachew Amogne, Sileshi Bantayehu
Department of Anesthesia, College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia.
Department of Anesthesiology, Vanderbilt University Medical Center, Nashville, TN, United States of America.
BMC Public Health. 2025 Aug 4;25(1):2641. doi: 10.1186/s12889-025-24034-y.
Multimorbidity, particularly prevalent among older patients, represents a growing global health challenge. This study investigates the prevalence of multimorbidity and its relationship with perioperative outcomes among older patients undergoing major surgery in Ethiopia.
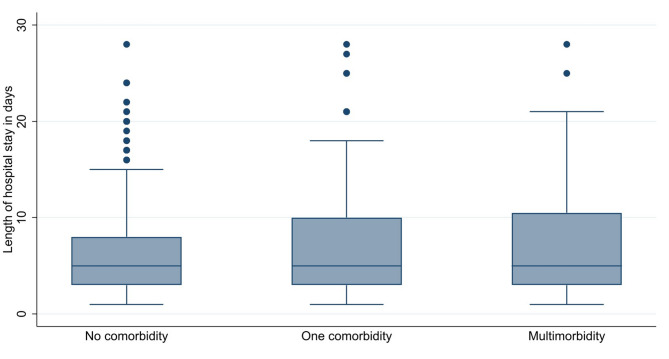
This longitudinal study was conducted at a tertiary teaching hospital in Northwest Ethiopia from June 01, 2019, to June 30, 2021. All consecutive older (aged 50+) patients who underwent major surgery during the study period were included. The primary outcome measure was estimating the prevalence of multimorbidity. Secondary outcome measures were the association between multimorbidity and 28-day perioperative mortality and length of hospital stay. A bivariable and multivariable modified Poisson regression was used to compute crude and adjusted relative risks, respectively, along with 95% confidence intervals (CIs) to assess the strength of association while adjusting for confounding covariates. A p-value < 0.05 was used to declare statistical significance.
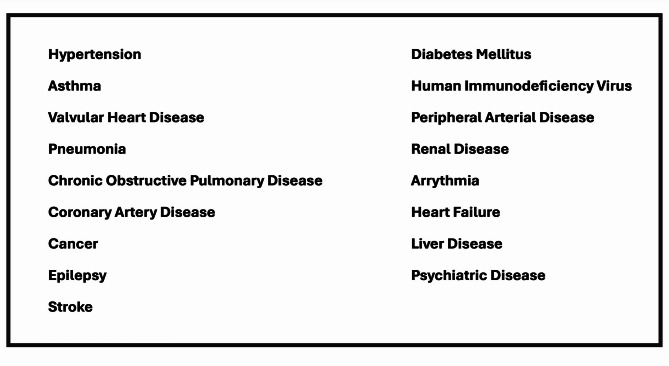
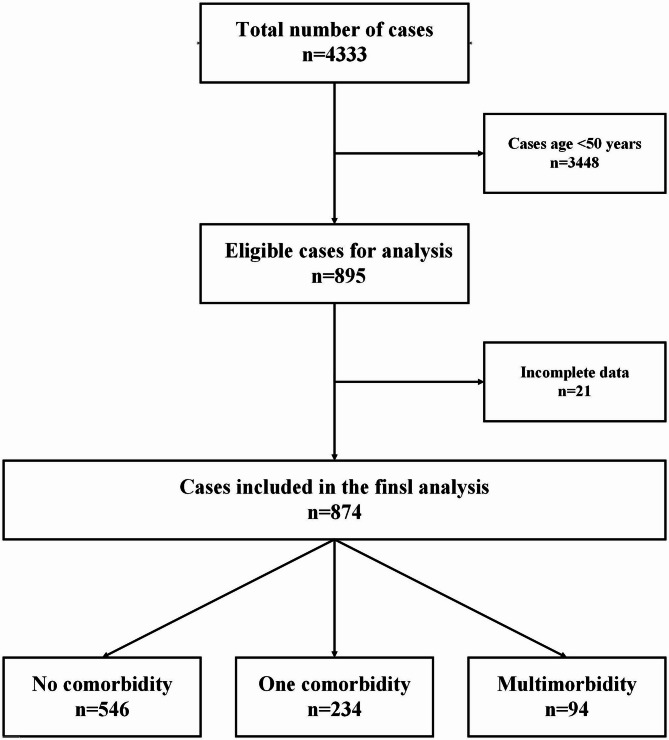
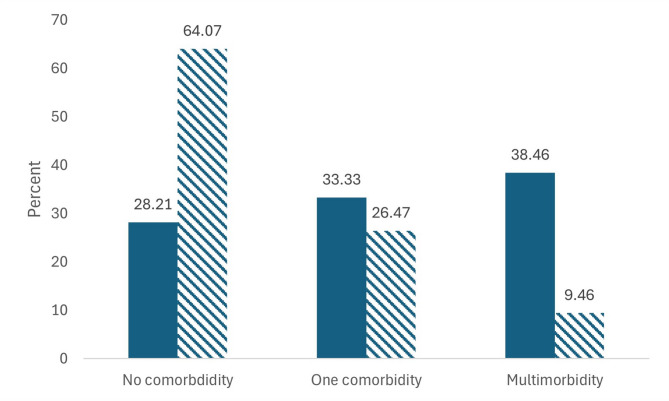
Of 874 patients who underwent major surgery, 234 (26.77%) patients had one comorbidity, and 94 (10.76%) patients had multimorbidity. Among all geriatric patients, 130 (14.87%) had hypertension, 34 (3.89%) had diabetes mellitus, and 29 (3.32%) had cancer. The most common multimorbidity combination was hypertension and diabetes (18 cases). The rates of perioperative mortality were higher in patients with multimorbidity compared with those with either one or no comorbidity (36.46% vs. 33.33% vs. 28.21%; p < 0.001). The risk of perioperative mortality after surgery among patients with multimorbidity was more than eight (adjusted relative risk = 8.07, 95% CI:2.39, 27.23) times higher than that of those with no comorbidity.
Multimorbidity in older surgical patients was common, and one in ten older patients undergoing major surgery had multimorbidity. Multimorbidity increases the risk of mortality among older patients following major surgery. We recommend targeted management of older surgical patients with multimorbidity by preoperative screening and optimization before surgery.
多病共存现象在老年患者中尤为普遍,是全球日益严峻的健康挑战。本研究调查了埃塞俄比亚接受大手术的老年患者中多病共存的患病率及其与围手术期结局的关系。
本纵向研究于2019年6月1日至2021年6月30日在埃塞俄比亚西北部的一家三级教学医院进行。纳入研究期间所有连续接受大手术的老年(50岁及以上)患者。主要结局指标是评估多病共存的患病率。次要结局指标是多病共存与28天围手术期死亡率及住院时间之间的关联。采用双变量和多变量修正泊松回归分别计算粗相对风险和调整后相对风险,并计算95%置信区间(CI),以评估关联强度,同时对混杂协变量进行校正。P值<0.05表示具有统计学意义。
在874例接受大手术的患者中,234例(26.77%)患者患有一种合并症,94例(10.76%)患者患有多病共存。在所有老年患者中,130例(14.87%)患有高血压,34例(3.89%)患有糖尿病,29例(3.32%)患有癌症。最常见的多病共存组合是高血压和糖尿病(18例)。多病共存患者的围手术期死亡率高于患有一种合并症或无合并症的患者(36.46%对33.33%对28.21%;P值<0.001)。多病共存患者术后围手术期死亡风险比无合并症患者高出八倍多(调整后相对风险=8.07,95%CI:2.39,27.23)。
老年手术患者中多病共存情况常见,每十名接受大手术的老年患者中就有一名患有多病共存。多病共存增加了老年患者大手术后的死亡风险。我们建议通过术前筛查和术前优化对患有多病共存的老年手术患者进行针对性管理。