Takano Hayabusa, Hara Naoki, Nakajima Eri, Katsuda Kouhei, Usami Kenki, Hasegawa Ayaka, Matsuda Jun, Arino Satoshi, Sasaki Nobuo, Kojima Naoki, Inagawa Hiroshi, Okada Yasusei, Fujita Akira
Department of Critical Care and Emergency Medicine, Showa General Hospital, Tokyo, Japan.
Department of Hematology, Showa General Hospital, Tokyo, Japan.
AME Case Rep. 2025 Jul 15;9:105. doi: 10.21037/acr-25-25. eCollection 2025.
Immune thrombocytopenia (ITP) is characterized by decreased platelet count due to immunological mechanisms. First-line treatment is corticosteroids, with thrombopoietin receptor agonists, rituximab, and splenectomy as second-line options. While surgical splenectomy is effective, it poses high bleeding risks in severe thrombocytopenia. Splenic embolization (SE) is considered an alternative to splenectomy for the treatment of steroid-refractory chronic ITP and has been reported to be an effective and minimally invasive option. However, there are few reports of SE being performed for acute ITP with life-threatening bleeding.
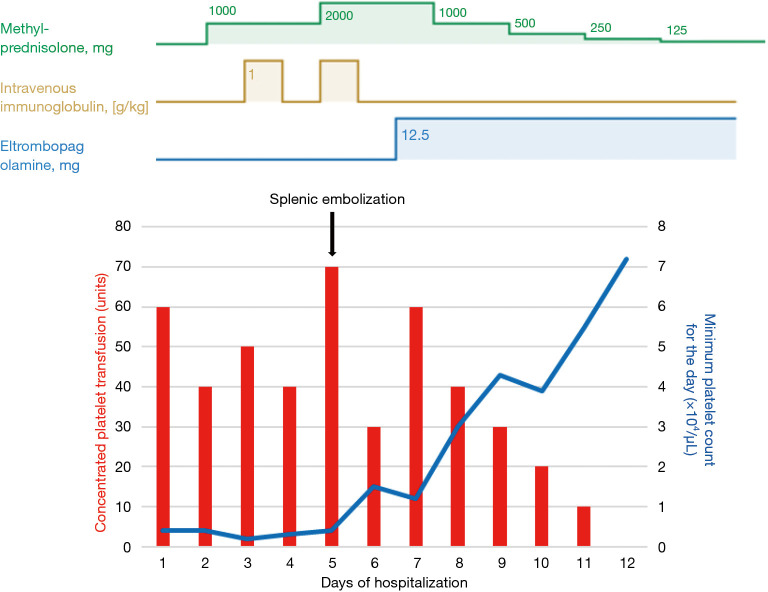
A 63-year-old man presented in shock with oral bleeding, bloody stools, and recurrent syncope. Laboratory tests revealed severe thrombocytopenia (4,000/mm platelets) and elevated platelet-associated immunoglobulin G (PA-IgG), leading to ITP diagnosis. Despite platelet transfusions, intravenous immunoglobulin, and high-dose steroids, his condition worsened with alveolar hemorrhage developing on day 3. Given the surgical risks, emergency SE was performed on day 5 using coils and gelatin sponge. Following SE and thrombopoietin receptor agonist administration, platelet counts improved from day 6, allowing discontinuation of transfusions by day 11. The patient was discharged from the intensive care unit on day 12 with stabilized platelets and improved respiratory status.
This case demonstrates that emergency SE can be an effective and safe alternative to splenectomy for refractory ITP with life-threatening bleeding, particularly when severe thrombocytopenia precludes surgical intervention. The rapid improvement in platelet counts suggests SE could be a viable emergency treatment option.
免疫性血小板减少症(ITP)的特征是由于免疫机制导致血小板计数减少。一线治疗是使用皮质类固醇,血小板生成素受体激动剂、利妥昔单抗和脾切除术作为二线选择。虽然手术脾切除术有效,但在严重血小板减少症中存在高出血风险。脾栓塞术(SE)被认为是治疗类固醇难治性慢性ITP的脾切除术替代方法,并且据报道是一种有效且微创的选择。然而,很少有关于对伴有危及生命出血的急性ITP进行SE的报道。
一名63岁男性因口腔出血、便血和反复晕厥而出现休克。实验室检查显示严重血小板减少(血小板计数为4000/mm)和血小板相关免疫球蛋白G(PA-IgG)升高,导致ITP诊断。尽管进行了血小板输注、静脉注射免疫球蛋白和高剂量类固醇治疗,但他的病情在第3天因肺泡出血而恶化。鉴于手术风险,在第5天使用线圈和明胶海绵进行了紧急SE。在SE和给予血小板生成素受体激动剂后,血小板计数从第6天开始改善,到第11天可以停止输血。患者在第12天从重症监护病房出院,血小板稳定,呼吸状况改善。
该病例表明,对于伴有危及生命出血的难治性ITP,紧急SE可以是脾切除术的有效且安全的替代方法,特别是当严重血小板减少症排除手术干预时。血小板计数的快速改善表明SE可能是一种可行的紧急治疗选择。