Zhu Qin, Huang Shaochen
Division of Kinesiology and Health, University of Wyoming, Laramie, WY, United States.
School of Health Promotion and Kinesiology, Texas Woman's University, 1600 N Bell Ave, Pioneer Hall, Denton, TX, 76209, United States, 1 940-898-2592.
Interact J Med Res. 2025 Aug 5;14:e70867. doi: 10.2196/70867.
Concussion has been a major public health concern due to the substantial cognitive sequelae it results. Although the dysfunctions of the frontal lobe and corpus callosum owing to concussions have been documented, the existing concussion screening tools merely examine cognitive functions in isolation of motor functions and failed to detect the chronic cognitive-motor impairments following concussions. Yet, there has been no concussion screening test aimed specifically to assess the coupled cognitive-motor functions.
This study aimed to provide preliminary evidence for using computerized eye-hand coordination tasks to detect chronic cognitive-motor deficits associated with concussion history.
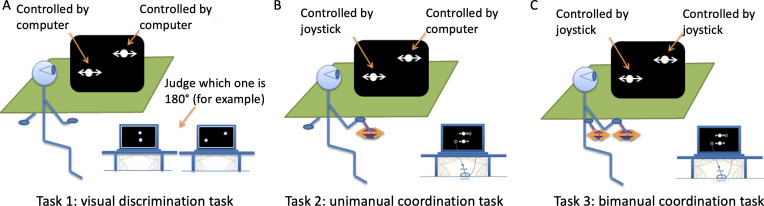
The computerized eye-hand coordination tasks were used to assess the coupled cognitive-motor functions of the participants with and with no history of concussion. In experiment 1, a total of 12 participants (6 young adults with a history of concussion and 6 healthy controls) completed longitudinal assessments of coordination profiles across a year. Experiment 2 examined a total of 20 participants (10 participants with a history of concussion and 10 healthy controls) using an iterated single-session protocol. Just noticeable difference (JND) and proportion of time-on-task (PTT) were used to assess cognitive-motor performance. Mixed-design ANOVAs were used to examine group differences, and the effect sizes were assessed using Cohen d test.
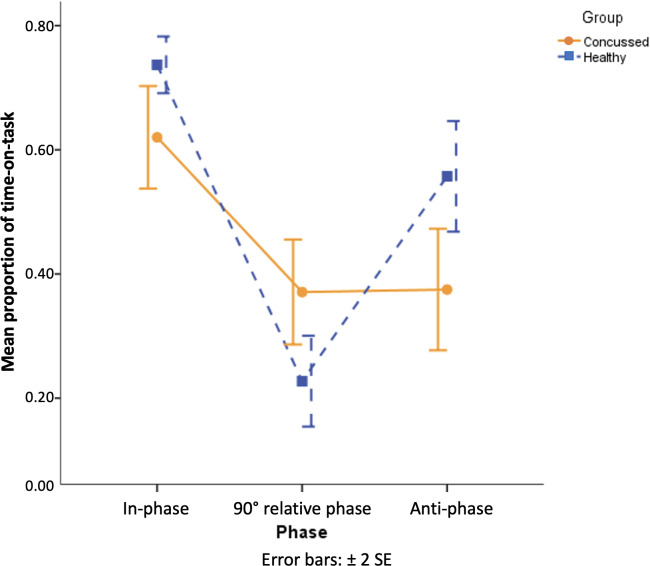
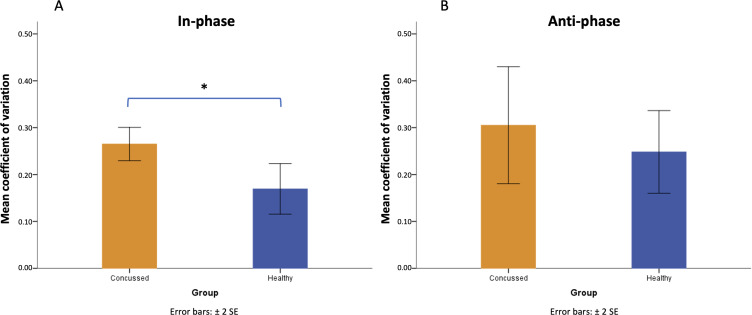
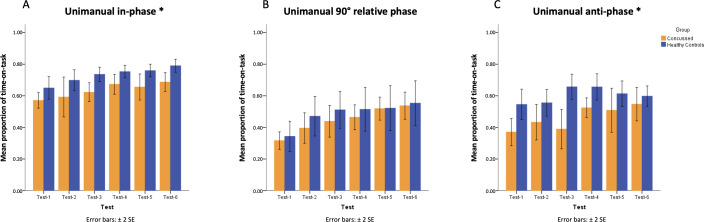
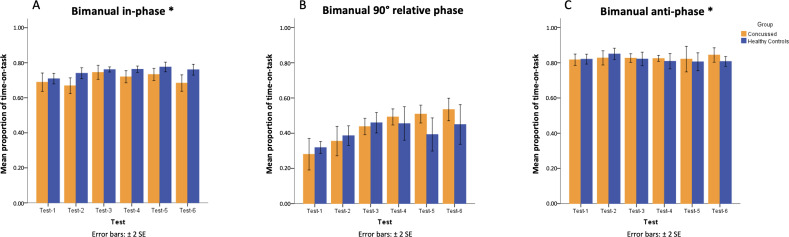
In experiment 1, participants with a history of concussion exhibited more inconsistent ability to visually discriminate the in-phase coordination pattern (coefficient of variation of JND: participants with a history of concussion = mean 0.27, SD 0.04, and healthy controls = mean 0.17, SD 0.07; t10=2.93; P=.02). Similarly, their performance on unimanual and bimanual in-phase and anti-phase coordination patterns was significantly poorer (at in-phase: PTTConcussed=mean 0.63, SD 0.10, and PTTHealthy=mean 0.73, SD 0.08 [F1,10=8.49; P=.02]; at anti-phase: PTTConcussed=mean 0.46, SD 0.14, and PTTHealthy=mean 0.60, SD 0.10 [F1,10=10.67; P=.008]). In experiment, 2 where only the unimanual coordination tasks were implemented for screening, participants with a history of concussion showed impaired performance in both in-phase and anti-phase tasks (at in-phase: PTTConcussed=mean 0.62, SD 0.13, and PTTHealthy=mean 0.74, SD 0.07 [F1,54=4.20; P=.045]; at anti-phase: PTTConcussed=mean 0.37, SD 0.15, and PTTHealthy=mean 0.56, SD 0.14 [F1,54=10.26; P=.002]), and they also failed to show the differentiated performance between anti-phase and 90° coordination patterns (PTTAnti-phase=mean 0.37, SD 0.15, and PTT90° coordination=mean 0.37, SD 0.13).
Due to their ability to detect both impaired and undifferentiated performance in producing intrinsic and novel coordination patterns, the unimanual coordination tasks appear to be a sensitive screening tool for chronic cognitive-motor deficits associated with history of concussion.
由于脑震荡会导致严重的认知后遗症,它一直是一个主要的公共卫生问题。尽管已有文献记载脑震荡会导致额叶和胼胝体功能障碍,但现有的脑震荡筛查工具仅孤立地检查认知功能,而未涉及运动功能,也未能检测出脑震荡后的慢性认知 - 运动障碍。然而,目前尚无专门针对评估联合认知 - 运动功能的脑震荡筛查测试。
本研究旨在为使用计算机化眼手协调任务检测与脑震荡病史相关的慢性认知 - 运动缺陷提供初步证据。
使用计算机化眼手协调任务评估有和无脑震荡病史参与者的联合认知 - 运动功能。在实验1中,共有12名参与者(6名有脑震荡病史的年轻人和6名健康对照)在一年时间内完成了协调特征的纵向评估。实验2采用重复单节段方案对总共20名参与者(10名有脑震荡病史的参与者和10名健康对照)进行了检查。使用最小可觉差(JND)和任务执行时间比例(PTT)来评估认知 - 运动表现。采用混合设计方差分析来检验组间差异,并使用Cohen d检验评估效应大小。
在实验1中,有脑震荡病史的参与者在视觉辨别同相协调模式时表现出更不一致的能力(JND的变异系数:有脑震荡病史的参与者 = 均值0.27,标准差0.04,健康对照 = 均值0.17,标准差0.07;t10 = 2.93;P = 0.02)。同样,他们在单手和双手同相及反相协调模式下的表现明显更差(同相时:PTT脑震荡组 = 均值0.63,标准差0.10,PTT健康组 = 均值0.73,标准差0.08 [F1,10 = 8.49;P = 0.02];反相时:PTT脑震荡组 = 均值0.46,标准差0.14,PTT健康组 = 均值0.60,标准差0.10 [F1,10 = 10.67;P = 0.008])。在实验2中,仅实施单手协调任务进行筛查,有脑震荡病史的参与者在同相和反相任务中均表现受损(同相时:PTT脑震荡组 = 均值0.62,标准差0.13,PTT健康组 = 均值0.74,标准差0.07 [F1,54 = 4.20;P = 0.045];反相时:PTT脑震荡组 = 均值0.37,标准差0.15,PTT健康组 = 均值0.56,标准差0.14 [F1,54 = 10.26;P = 0.002]),并且他们在反相和90°协调模式之间也未表现出差异(PTT反相 = 均值0.37,标准差0.15,PTT90°协调 = 均值0.37,标准差0.13)。
由于单手协调任务能够检测出在产生内在和新颖协调模式时受损及未分化的表现,它似乎是一种检测与脑震荡病史相关的慢性认知 - 运动缺陷的敏感筛查工具。