Zheng Hongcheng, Zeng Yongtao, Daoerji Nacke, Wang Husen, Tang Bin, Shu Li
The Sixth Affiliated Hospital of Xinjiang Medical University, Urumqi, Xinjiang, 86830001, China.
BMC Surg. 2025 Aug 5;25(1):339. doi: 10.1186/s12893-025-03101-6.
Anterior cruciate ligament (ACL) reconstruction remains the gold standard but carries donor-site morbidity and prolonged recovery. Modern ACL repair techniques theoretically preserve native proprioception and enable faster rehabilitation. We hypothesized that modern ACL repair would demonstrate non-inferior clinical outcomes compared to reconstruction.This meta-analysis compares clinical outcomes of primary repair versus autograft reconstruction.
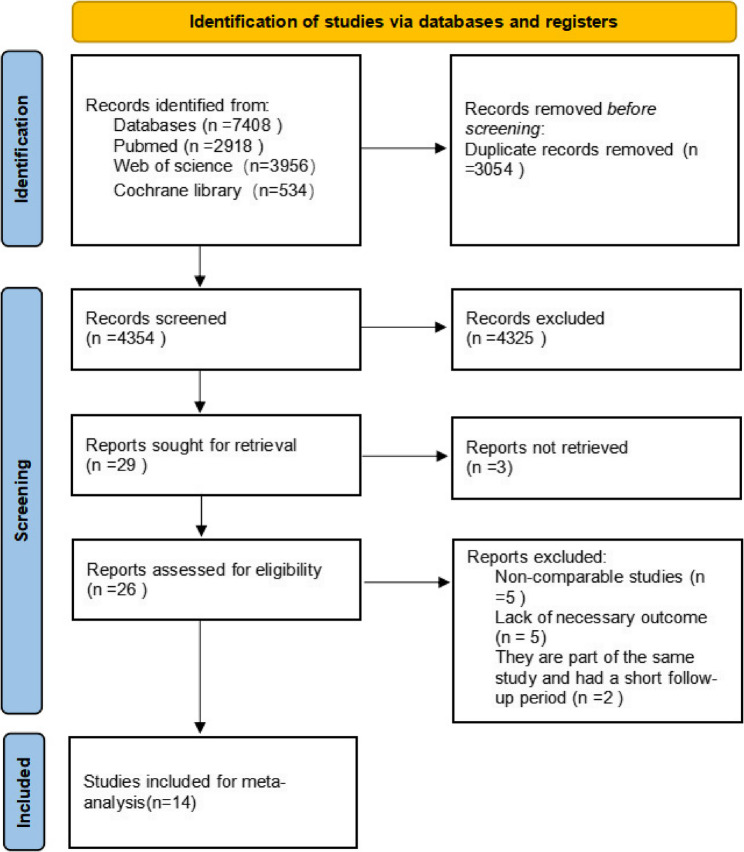
We systematically searched PubMed, Cochrane Library, and Web of Science (2015–2025) for comparative studies (RCTs, cohorts, case-controls) reporting ≥ 2 key outcomes (failure rate, AP knee laxity, IKDC, Lysholm, or Tegner scores) with ≥ 1-year follow-up. Pooled ORs and WMDs with 95% CIs were calculated using RevMan 5.4. Subgroup analyses (injury-to-surgery time, injury location, study design, repair technique) and GRADE assessment were performed.
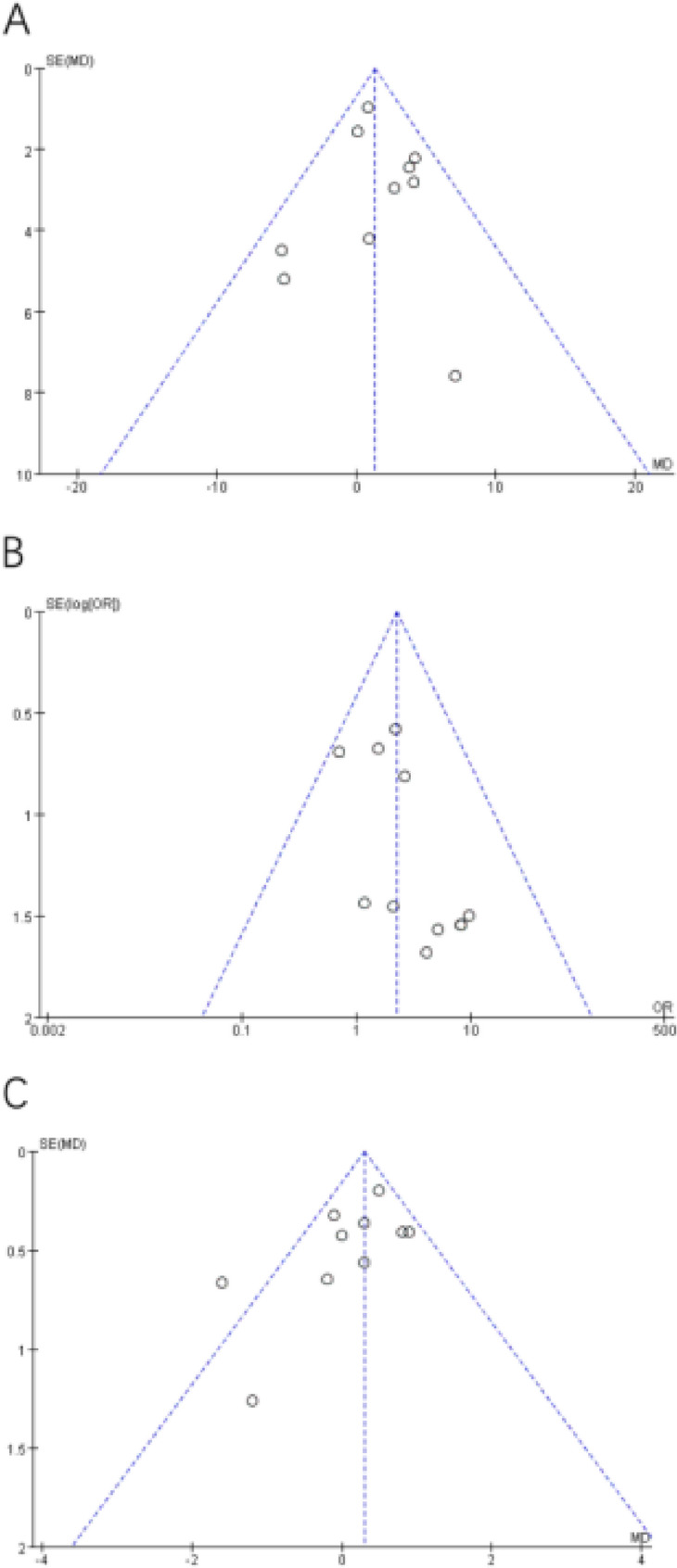
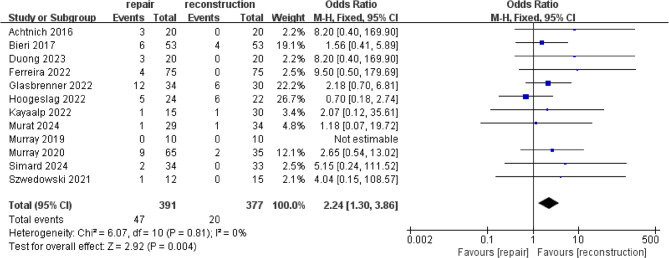
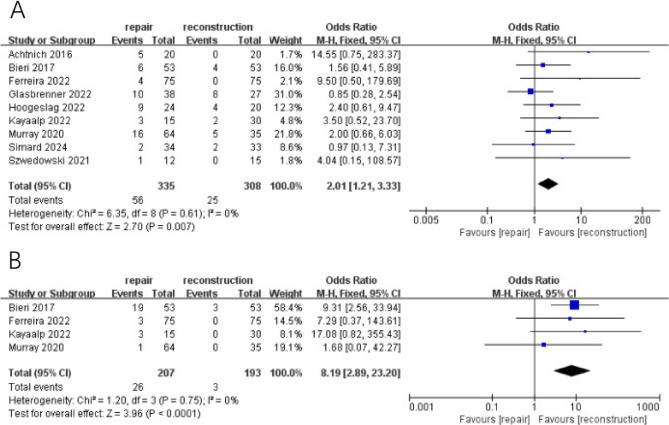
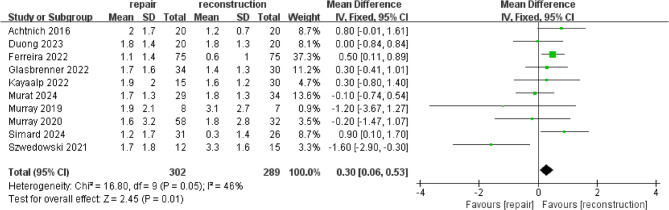
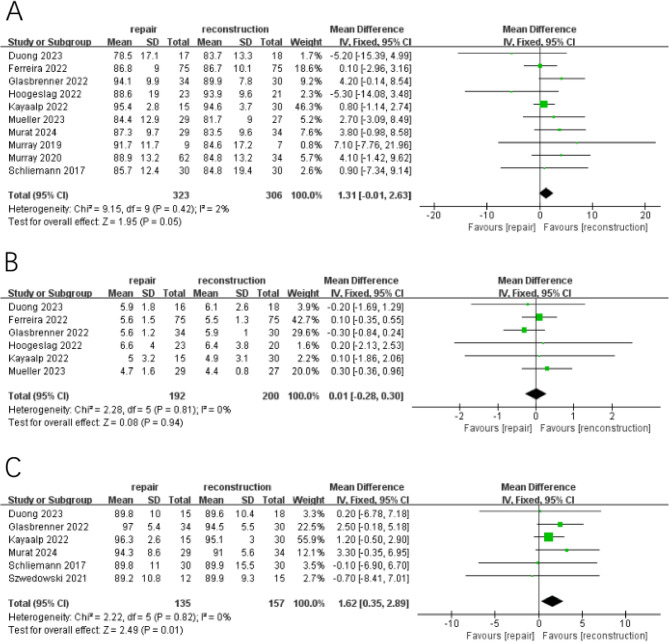
Fourteen studies (4 RCTs, 8 cohorts, 2 case-controls; = 908 patients) were included (repair: = 460; reconstruction: = 448). Failure/Revision Rates: Repair demonstrated numerically higher failure rates (OR = 2.24, 95% CI 1.30–3.86, = 0.004) and revision rates (OR = 2.01, 95% CI 1.21–3.33, = 0.007) versus reconstruction.Hardware removal: increased hardware removal incidence was observed in repair groups (OR = 8.19, 95% CI 2.89–23.20, < 0.001).AP knee laxity: reconstruction showed marginally lower AP knee laxity (WMD = 0.30, 95% CI 0.06–0.53, = 0.01).Patient-reported outcomes: no significant differences in IKDC (WMD = 1.31,95%CI: −0.01–2.63; = 0.05) or Tegner scores (WMD: 0.01; 95% CI: -0.28– 0.30; = 0.94). Lysholm scores slightly favored reconstruction (WMD = 1.62,; 95% CI: 0.35–2.89; = 0.01).Key subgroup findings: repair achieved comparable outcomes to reconstruction in: (1) RCT-designed studies, (2) Acute repairs (< 21 days post-injury).
ACL repair is associated with higher failure and revision rates than reconstruction overall, but may be a viable alternative in selected patients with acute proximal tears.
The online version contains supplementary material available at 10.1186/s12893-025-03101-6.
前交叉韧带(ACL)重建仍是金标准,但会带来供区并发症和恢复时间延长的问题。现代ACL修复技术理论上可保留天然本体感觉并实现更快的康复。我们假设现代ACL修复与重建相比将显示出非劣效的临床结果。本荟萃分析比较了初次修复与自体移植重建的临床结果。
我们系统检索了PubMed、Cochrane图书馆和科学网(2015 - 2025年),以查找报告≥2项关键结果(失败率、膝关节前后向松弛度、国际膝关节文献委员会(IKDC)评分、Lysholm评分或Tegner评分)且随访≥1年的比较研究(随机对照试验、队列研究、病例对照研究)。使用RevMan 5.4计算合并的比值比(OR)和加权均数差(WMD)以及95%可信区间(CI)。进行了亚组分析(受伤至手术时间、损伤部位、研究设计、修复技术)和GRADE评估。
纳入了14项研究(4项随机对照试验、8项队列研究、2项病例对照研究;n = 908例患者)(修复组:n = 460;重建组:n = 448)。失败/翻修率:与重建相比,修复显示出数值上更高的失败率(OR = 2.24,95%CI 1.30 - 3.86,P = 0.004)和翻修率(OR = 2.01,95%CI 1.21 - 3.33,P = 0.007)。取出内植物:修复组观察到取出内植物的发生率增加(OR = 8.19,95%CI 2.89 - 23.20,P < 0.001)。膝关节前后向松弛度:重建显示膝关节前后向松弛度略低(WMD = 0.30,95%CI 0.06 - 0.53,P = 0.01)。患者报告的结果:IKDC评分(WMD = 1.31,95%CI:−0.01 - 2.63;P = 0.05)或Tegner评分(WMD:0.01;95%CI: - 0.28 - 0.30;P = 0.94)无显著差异。Lysholm评分略倾向于重建(WMD = 1.62;95%CI:0.35 - 2.89;P = 0.01)。关键亚组发现:在以下情况中,修复与重建取得了可比的结果:(1)随机对照试验设计的研究,(2)急性修复(受伤后<21天)。
总体而言,ACL修复与重建相比失败率和翻修率更高,但对于某些急性近端撕裂的患者可能是一种可行的替代方法。
在线版本包含可在10.1186/s12893 - 025 - 03101 - 6获取的补充材料。