El-Halabi Soha, Pembe Andrea Barnabas, Dumont Alexandre, Betrán Ana Pilar, Kaboré Charles, Chipeta Effie, Carroli Guillermo, Alvesson Helle Mölsted, Kidanto Hussein, Dossou Jean-Paul, Annerstedt Kristi Sidney, Beňová Lenka, Gross Mechthild M, Waiswa Peter, Lumbiganon Pisake, Mac Quoc Nhu Hung, Bohren Meghan A, Hanson Claudia
Department of Global Public Health, Karolinska Institutet, Stockholm, Sweden.
Department of Obstetrics and Gynaecology, College of Medicine, Muhimbili University of Health and Allied Sciences, Dar Es Salaam, Tanzania.
Front Health Serv. 2025 Jul 23;5:1550473. doi: 10.3389/frhs.2025.1550473. eCollection 2025.
Labor companionship, the presence of a woman's person of choice during childbirth, has benefits to both woman and baby and is recommended by the World Health Organization since 2012. However, implementation remains sub-optimal, especially in low-and-middle-income countries (LMICs). This study aimed to understand the maturity of labor companionship implementation in eight low-and-middle income countries with focus on the policy and facility environment.
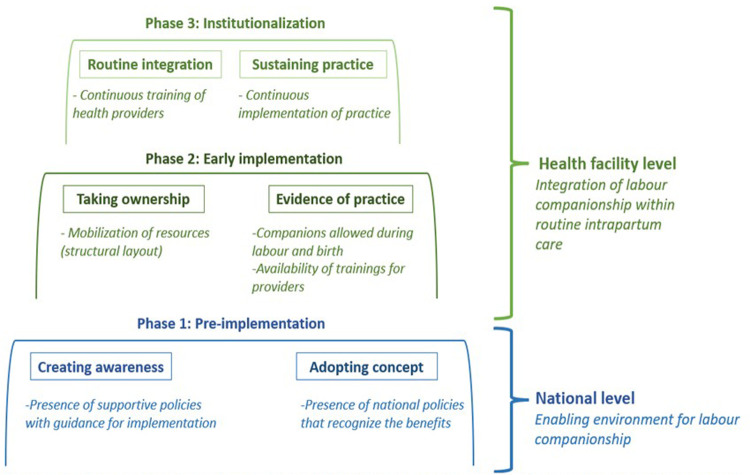
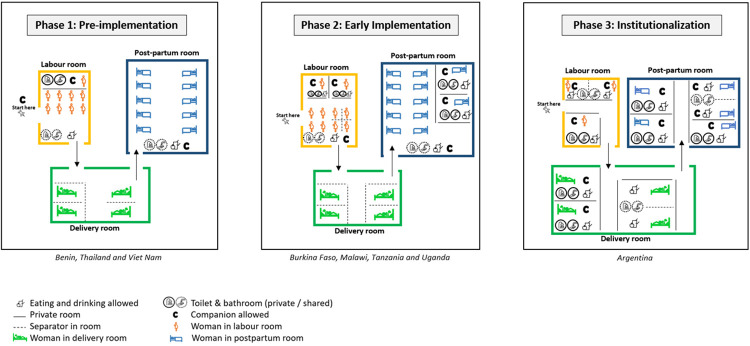
This was a multi-country study nested in two hospital-based implementation research studies: Action Leveraging Evidence to Reduce perinatal mortality and morbidity in Sub-Saharan Africa (ALERT) study and the QUALIty DECision-making by women and providers for appropriate use of caesarean section (QUALI-DEC) study. We included 48 hospitals from eight countries: Argentina, Burkina Faso, Thailand and Viet Nam (QUALI-DEC) and four from each of Benin, Malawi, Tanzania and Uganda (ALERT). We used data from (i) a document review, including national policy documents and (ii) health facility readiness assessment, including physical layouts of maternity wards, all collected between December 2019 and April 2021. Our analysis included two steps, (1) a structured data abstraction with coding to pre-defined categories to analyse the national polices and available resources on a facility level which informed the (2) categorization of implementation maturity in three implementation phases modelled by the framework by Bergh et al. and the logic model developed by Bohren et al.
Three of the eight countries lacked any national-level companionship policies, four had some mentioning and only one had detailed guidance on roles of labor companions and implementation guidelines. The physical outlines of maternity wards varied greatly, and lack of space was one of the main implementation barriers to all countries except Argentina. We classified Benin, Thailand and Viet Nam in the pre-implementation phase because of missing guidelines and limited implementation; Burkina Faso, Malawi, Uganda and Tanzania in the early implementation phase; and Argentina in the institutionalization phase where policies and facility resources were conducive.
Successful implementation was supported by concrete and contextualized implementation guidance. To move to high implementation levels, supporting policies, guidelines and structural changes in the maternity wards are needed.
分娩陪伴,即在分娩期间有女性选择的人在场,对产妇和婴儿均有益处,自2012年起得到世界卫生组织的推荐。然而,其实施情况仍未达到最佳水平,尤其是在低收入和中等收入国家(LMICs)。本研究旨在了解八个低收入和中等收入国家分娩陪伴实施的成熟度,重点关注政策和机构环境。
这是一项嵌套在两项基于医院的实施研究中的多国研究:撒哈拉以南非洲利用证据减少围产期死亡率和发病率行动(ALERT)研究以及妇女和提供者进行剖宫产合理使用的质量决策(QUALI-DEC)研究。我们纳入了来自八个国家的48家医院:阿根廷、布基纳法索、泰国和越南(QUALI-DEC),以及贝宁、马拉维、坦桑尼亚和乌干达各四家(ALERT)。我们使用了(i)文件审查的数据,包括国家政策文件,以及(ii)医疗机构准备情况评估的数据,包括产科病房的物理布局,所有数据均在2019年12月至2021年4月期间收集。我们的分析包括两个步骤,(1)进行结构化数据提取并编码到预定义类别,以分析国家政策和机构层面的可用资源,这为(2)根据伯格等人的框架和博伦等人开发的逻辑模型所构建的三个实施阶段对实施成熟度进行分类提供了依据。
八个国家中有三个国家缺乏任何国家级的陪伴政策,四个国家有一些提及,只有一个国家对分娩陪伴者的角色和实施指南有详细指导。产科病房的物理布局差异很大,除阿根廷外,空间不足是所有国家的主要实施障碍之一。由于缺乏指南且实施有限,我们将贝宁、泰国和越南归类为实施前阶段;布基纳法索、马拉维、乌干达和坦桑尼亚归类为早期实施阶段;阿根廷归类为制度化阶段,其政策和机构资源较为有利。
具体且因地制宜的实施指南有助于成功实施。要达到高实施水平,需要支持性政策、指南以及产科病房的结构变革。