Kistner Anna, Alagic Zlatan, Enocson Anders, Koskinen Seppo K
Department of Molecular Medicine and Surgery, Karolinska Institute, Stockholm, 171 77, Sweden.
Department of Nuclear Medicine and Medical Physics, Karolinska University Hospital, Stockholm, 171 76, Sweden.
Sci Rep. 2025 Aug 7;15(1):28972. doi: 10.1038/s41598-025-14113-w.
Our purpose was to assess the prevalence of liver injuries as well as concomitant injuries to the liver and spleen in patients with blunt or penetrating abdominal trauma, and to determine the prevalence, management and outcome of active bleeding and contained vascular injuries (CVI; pseudoaneurysm/AV-fistula) seen on admission CT. A retrospective, single-center, longitudinal cohort study with nine-year data (2013-2021) of all ≥ 15-year-old patients with severe blunt or penetrating abdominal trauma and an ICD code for liver and/or splenic trauma. CT examinations were identified. Radiology, medical reports and images were reviewed and only patients with an adequate admission CT were included in the final study group. Of 2805 patients with abdominal trauma (71% males), 409 patients (14.6%) had a liver injury, and 329 had a CT on admission (329/409; 80.4%). 313 patients (11.2%) had a splenic injury and 262 had a CT (262/313; 83.7%). Of these, 65 patients or 2.3% (65/2805) had injury to both organs, with 49 patients with CT (49/65; 75.4%), combined group (CG) (79% males). The median (range) ISS was 21 (4-75) for single organ injury patients and 34 (9-75) for patients with both organs injured (p < 0.0001). Active liver or splenic bleeding was seen in 5.8% and 17.9%, respectively. In CG, 11 (11/49; 22.4%) patients had active bleeding. Of these, two patients had active bleeing in both organs (4.1%). Liver patients with active bleeding had significantly higher ISS (p = 0.025) than those without. In CG, ISS did not differ significantly between patients with and without active bleeding (p = 0.073), however, it tended to be higher in those with active bleeding. Most liver injuries with active bleeding were treated non-operatively (12/19; 63.2%). An active bleeding was more common in spleen than in liver patients; odds ratio (OR) (95% CI) 3.57 (2.04-6.25), p < 0.0001. A CVI was more common in splenic compared with liver injuries, OR 6.71 (95% CI; 2.27-19.9, p < 0.0001). Active bleeding was more common in CG than in single organ injury patients; OR 3.67 (1.73-7.79), p < 0.0016. 30-day survival rate did not differ between patients with or without active bleeding, but was slightly lower in CG compared with only liver injury (89.8% vs. 93.7%, p = 0.36). In conclusion the prevalence of liver injury in abdominal trauma seen on admission CT was 11.7% of all patients with blunt or penetrating abdominal trauma, and concomitant splenic and liver injury was seen in 1.7%. Non-operative management was applied in almost two thirds of patients with liver injuries. Active bleeding was seen in 5.8% of liver, 17.9% of splenic and 22.4% of CG patients. ISS was doubled in CG compared with single organ injury patients. Active bleeding was more common in CG, and CG had slightly increased mortality rate compared with single organ injury patients.
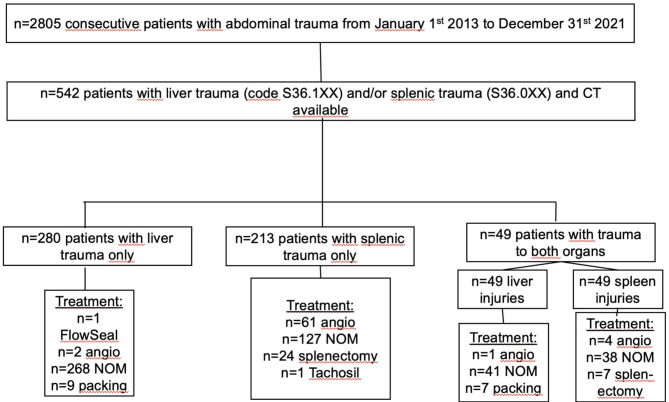
我们的目的是评估钝性或穿透性腹部创伤患者肝脏损伤以及肝脏和脾脏合并损伤的发生率,并确定入院时CT所见活动性出血和局限性血管损伤(CVI;假性动脉瘤/动静脉瘘)的发生率、处理方法及预后。这是一项回顾性、单中心、纵向队列研究,纳入了2013年至2021年期间所有年龄≥15岁、患有严重钝性或穿透性腹部创伤且有肝脏和/或脾脏创伤ICD编码的患者。通过检索CT检查资料进行研究。回顾了放射学、医学报告及影像资料,最终研究组仅纳入入院时CT检查合格的患者。在2805例腹部创伤患者中(男性占71%),409例(14.6%)有肝脏损伤,其中329例入院时进行了CT检查(329/409;80.4%)。313例(11.2%)有脾脏损伤,262例进行了CT检查(262/313;83.7%)。其中,65例患者(2.3%,65/2805)两个器官均有损伤,49例进行了CT检查(49/65;75.4%),为联合损伤组(CG)(男性占79%)。单器官损伤患者的损伤严重度评分(ISS)中位数(范围)为21(4 - 75),两个器官均损伤患者的ISS中位数(范围)为34(9 - 75)(p < 0.0001)。肝脏或脾脏活动性出血的发生率分别为5.8%和17.9%。在联合损伤组中,11例(11/49;22.4%)患者有活动性出血。其中,2例患者两个器官均有活动性出血(4.1%)。有活动性出血的肝脏损伤患者的ISS显著高于无活动性出血者(p = 0.025)。在联合损伤组中,有活动性出血和无活动性出血患者的ISS差异无统计学意义(p = 0.073),但有活动性出血者的ISS有升高趋势。大多数有活动性出血的肝脏损伤采用非手术治疗(12/19;63.2%)。脾脏损伤患者中活动性出血比肝脏损伤患者更常见;优势比(OR)(95%置信区间)为3.57(2.04 - 6.25),p < 0.0001。与肝脏损伤相比,CVI在脾脏损伤中更常见,OR为6.71(95%置信区间;2.27 - 19.9,p < 0.0001)。联合损伤组中活动性出血比单器官损伤患者更常见;OR为3.67(1.73 - 7.79),p < 0.0016。有或无活动性出血患者的30天生存率无差异,但联合损伤组与仅肝脏损伤患者相比略低(89.8%对93.7%,p = 0.36)。总之,入院时CT所见腹部创伤患者中肝脏损伤的发生率为所有钝性或穿透性腹部创伤患者的11.7%;肝脏和脾脏合并损伤的发生率为1.7%。近三分之二的肝脏损伤患者采用非手术治疗。肝脏损伤患者中活动性出血的发生率为5.8%,脾脏损伤患者中为17.9%,联合损伤组中为22.4%。与单器官损伤患者相比,联合损伤组患者的ISS翻倍。联合损伤组中活动性出血更常见,且与单器官损伤患者相比,联合损伤组死亡率略有升高。

