Liu Ruifeng, Gao Xiangyu, Fan Jihong, Zhao Huiqiang
Department of Cardiology, Beijing Friendship Hospital Affiliated to Capital Medical University, 100050 Beijing, China.
Rev Cardiovasc Med. 2025 Jul 22;26(7):37301. doi: 10.31083/RCM37301. eCollection 2025 Jul.
Ventricular fibrillation (VF) is a life-threatening complication of acute myocardial infarction (AMI), particularly in patients undergoing percutaneous coronary intervention (PCI). Early identification of high-risk patients is crucial for implementing preventive measures and improving outcomes.
This retrospective study analyzed clinical, laboratory, and angiographic data from 155 AMI patients to identify predictors of VF during PCI. Variable selection was performed using least absolute shrinkage and selection operator (LASSO) regression, elastic net regression, and random forest. Independent predictors were identified through multivariable logistic regression, and a nomogram was developed and validated to predict VF risk. Model performance was assessed using receiver operating characteristic (ROC) and calibration curves.
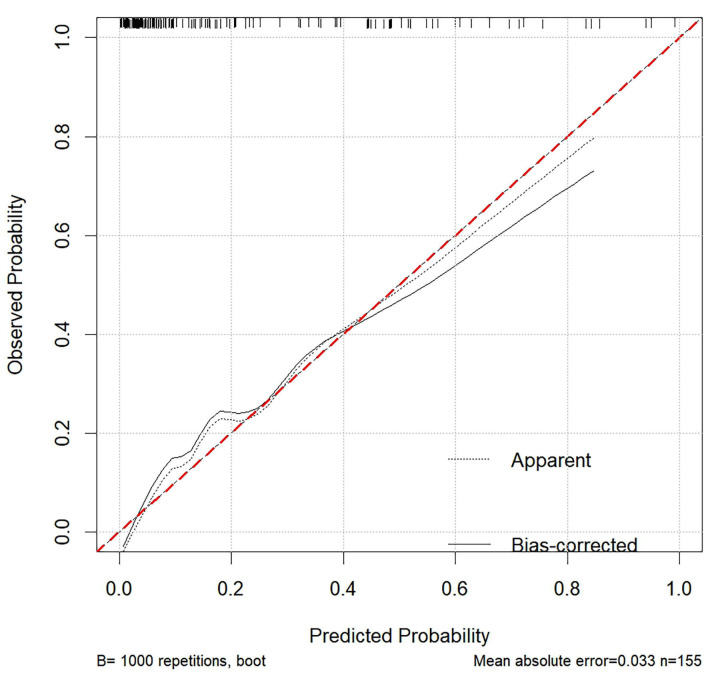
Independent predictors of VF included diabetes (OR = 3.676 (1.365-10.668); = 0.012), neutrophil-to-lymphocyte ratio (NLR) (odds ratio (OR) = 1.149 (1.053-1.265); = 0.002), right coronary artery (RCA) intervention (OR = 3.185 (1.088-9.804); = 0.037), Gensini score (OR = 1.020 (1.007-1.033); = 0.003), and absence of beta blockers (OR = 0.168 (0.054-0.472); = 0.001). The nomogram, incorporating these predictors, demonstrated a strong discriminative ability with an area under the ROC curve (AUC) of 0.882 (0.825-0.939) and good calibration (Hosmer-Lemeshow test, = 0.769). The calibration curve showed a strong alignment between predicted probabilities and observed outcomes, with a mean absolute error of 0.033.
This study identified diabetes, NLR, RCA intervention, Gensini score, and absence of beta-blocker use as key predictors of VF during PCI in AMI patients. A nomogram incorporating these factors showed strong predictive performance, aiding clinicians in identifying high-risk patients for targeted preventive strategies.
心室颤动(VF)是急性心肌梗死(AMI)的一种危及生命的并发症,尤其是在接受经皮冠状动脉介入治疗(PCI)的患者中。早期识别高危患者对于实施预防措施和改善预后至关重要。
这项回顾性研究分析了155例AMI患者的临床、实验室和血管造影数据,以确定PCI期间VF的预测因素。使用最小绝对收缩和选择算子(LASSO)回归、弹性网回归和随机森林进行变量选择。通过多变量逻辑回归确定独立预测因素,并开发和验证了一个列线图以预测VF风险。使用受试者工作特征(ROC)曲线和校准曲线评估模型性能。
VF的独立预测因素包括糖尿病(OR = 3.676(1.365 - 10.668);P = 0.012)、中性粒细胞与淋巴细胞比值(NLR)(比值比(OR) = 1.149(1.053 - 1.265);P = 0.002)、右冠状动脉(RCA)介入(OR = 3.185(1.088 - 9.804);P = 0.037)、Gensini评分(OR = 1.020(1.007 - 1.033);P = 0.003)以及未使用β受体阻滞剂(OR = 0.168(0.054 - 0.472);P = 0.001)。纳入这些预测因素的列线图显示出较强的判别能力,ROC曲线下面积(AUC)为0.882(0.825 - 0.939),校准良好(Hosmer-Lemeshow检验,P = 0.769)。校准曲线显示预测概率与观察结果之间高度一致,平均绝对误差为0.033。
本研究确定糖尿病、NLR、RCA介入、Gensini评分以及未使用β受体阻滞剂是AMI患者PCI期间VF的关键预测因素。纳入这些因素的列线图显示出强大的预测性能,有助于临床医生识别高危患者以制定针对性的预防策略。