Bayat Fariba, Tehrani Ramin Baghaei, Khani Mohammad, Akbari Tooba, Langroudi Taraneh Faghihi, Taheri Maryam, Alirezaei Amirhesam, Bagheri Amin, Ebrahimi Pouya
Cardiovascular Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Cardiac Surgery Department, School of Medicine, Modarres Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
J Cardiothorac Surg. 2025 Aug 9;20(1):329. doi: 10.1186/s13019-025-03566-9.
Right ventricle (RV) pseudoaneurysm is a substantially rare but fatal condition that should be diagnosed promptly to prevent severe complications, such as rupture and death. However, due to its nonspecific presentation, its diagnosis relies mainly on advanced imaging cardiac modalities. This report describes the successful management of a delayed and unusual presentation of RV pseudoaneurysm.
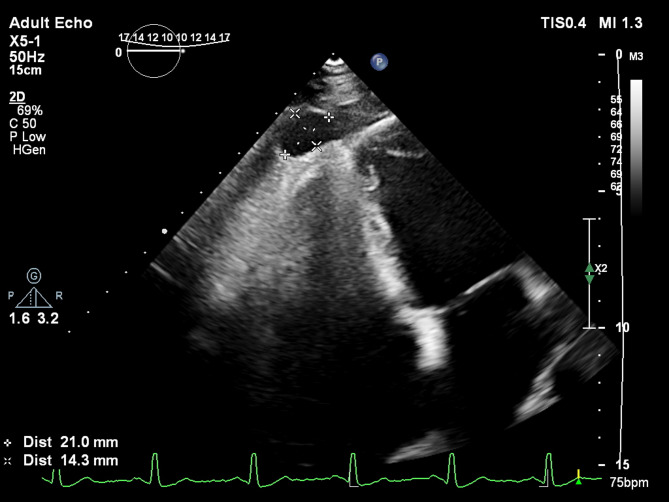
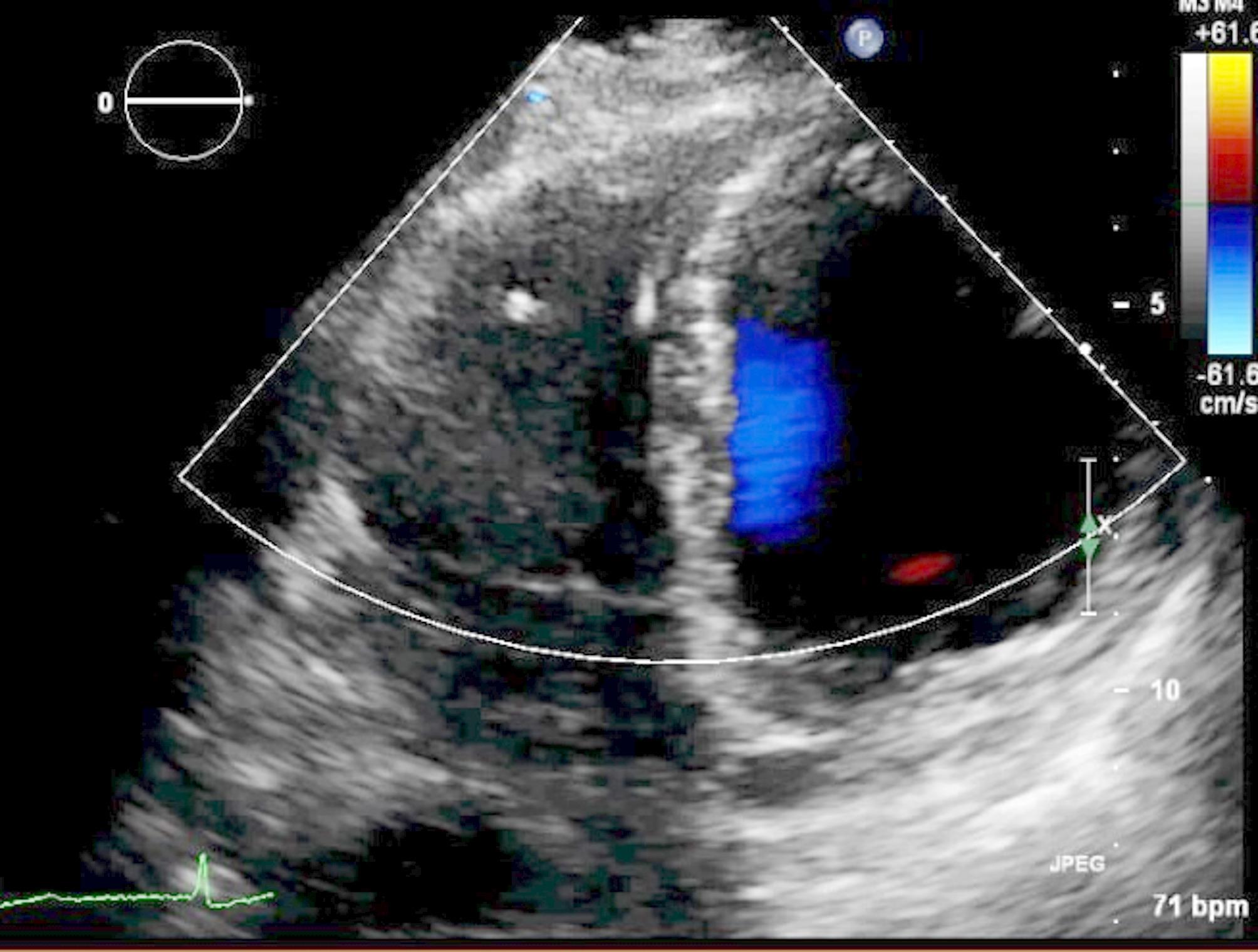
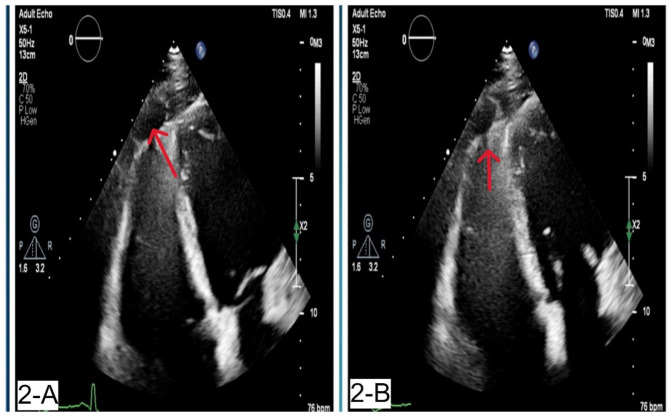
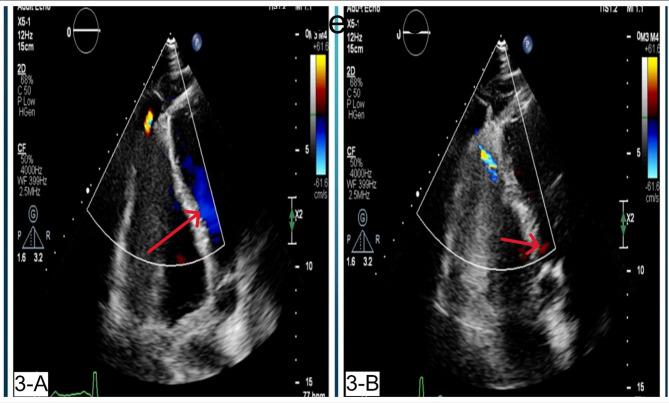
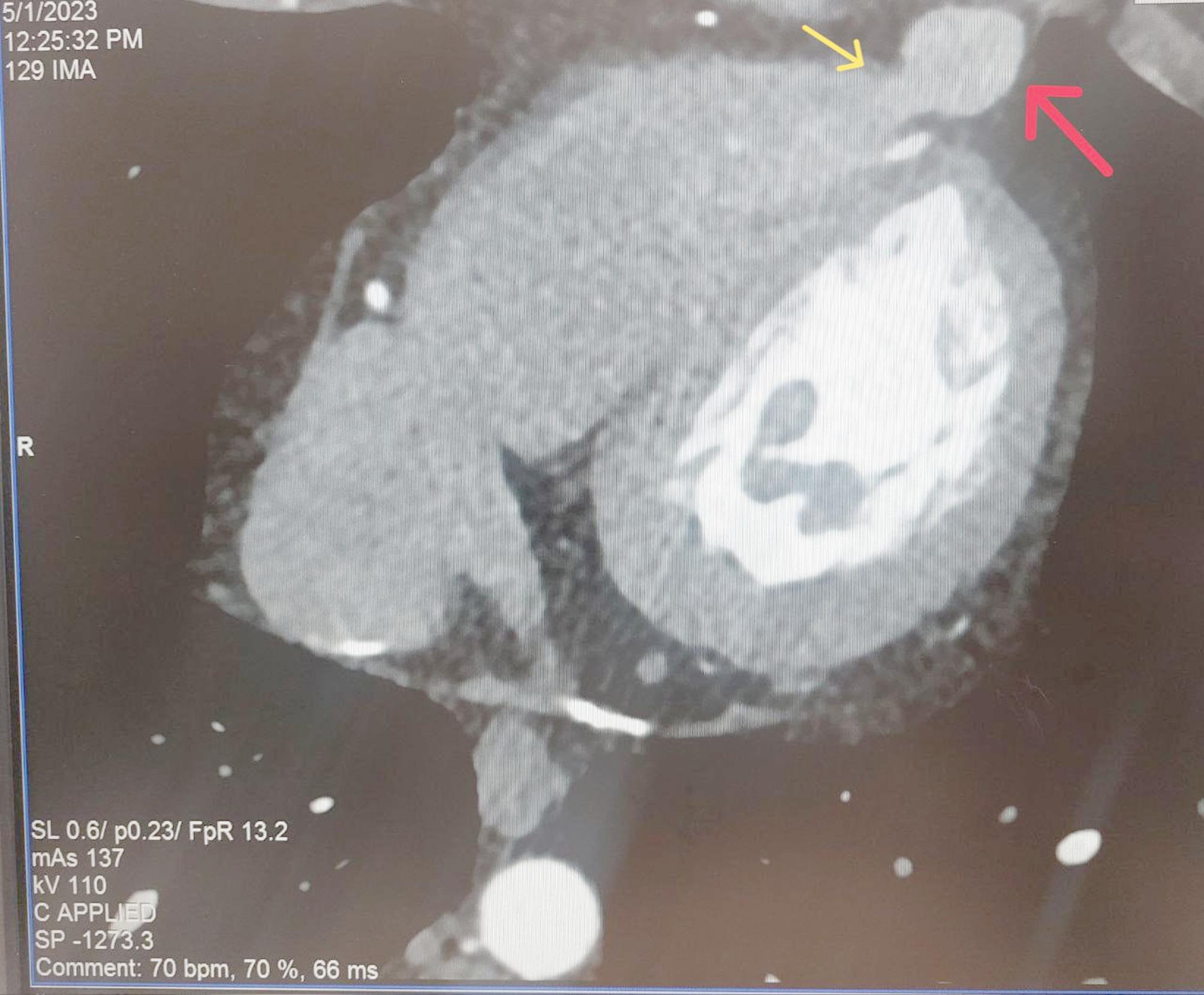
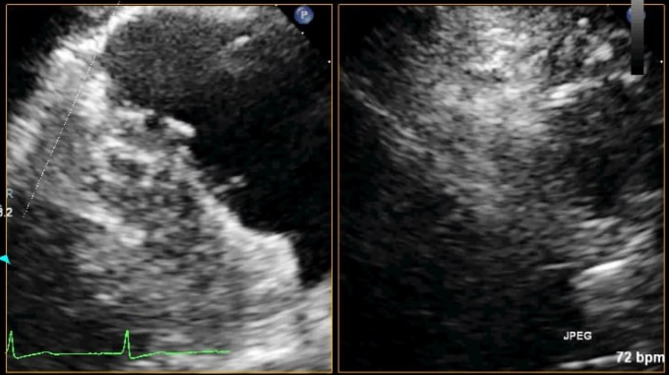
A 31-year-old white male patient with a history of pericardiectomy presented with chest pain and dyspnea, which worsened by exertion, and edema of the lower extremities, which had started several weeks ago and had been exacerbated over time. The initial evaluations with cardiac enzyme check, chest X-ray, and electrocardiogram were unremarkable, and the patient was planned to undergo a transthoracic echocardiogram (TTE). TTE revealed RV failure and increased RV diameter; a suspicious lesion in the RV apex was also detected, suggesting a pseudoaneurysm. Cardiac Computed Tomography (CTA) confirmed the diagnosis, and interventional treatment via an Amplatzer device was considered, which was rejected by the interventional cardiologist of the center due to the lack of experience and logistics for such intervention. Considering the patient's condition deterioration, the patient was transferred to an operating room, and an open-heart surgery was performed to suture the ruptured RV myocardium. The pericardial effusion was removed. The histopathological evaluation of the sample confirmed the diagnosis. The post-surgical recovery and follow-up were uneventful. The graphical abstract is added below to illustrate the case and summarize it.
CONCLUSION (CLINICAL KEY POINT): Right ventricle pseudoaneurysms can present with unusual symptoms and signs, and misdiagnosis is highly probable. Advanced imaging techniques after the initial echocardiogram might be necessary to confirm the diagnosis. Moreover, timely, appropriate, and wisely chosen treatment (interventional or surgical) can result in uneventful treatment and recovery.
右心室假性动脉瘤是一种极为罕见但致命的疾病,应及时诊断以预防诸如破裂和死亡等严重并发症。然而,由于其表现不具特异性,其诊断主要依赖于先进的心脏成像检查手段。本报告描述了一例延迟且不寻常表现的右心室假性动脉瘤的成功治疗。
一名31岁有心包切除术史的白人男性患者出现胸痛和呼吸困难,运动时加重,下肢水肿始于数周前且随时间加重。最初进行的心肌酶检查、胸部X线和心电图检查均无异常,计划对该患者进行经胸超声心动图(TTE)检查。TTE显示右心室功能衰竭且右心室直径增大;还在右心室心尖部检测到一个可疑病变,提示为假性动脉瘤。心脏计算机断层扫描(CTA)确诊了该诊断,考虑通过Amplatzer装置进行介入治疗,但该中心的介入心脏病专家因缺乏此类干预的经验和相关条件而拒绝了。鉴于患者病情恶化,将其转至手术室,进行了心脏直视手术以缝合破裂的右心室心肌。清除了心包积液。样本的组织病理学评估确诊了诊断。术后恢复和随访情况良好。下面添加了图形摘要以说明并总结该病例。
结论(临床要点):右心室假性动脉瘤可能表现出不寻常的症状和体征,极易误诊。初次超声心动图检查后可能需要先进的成像技术来确诊。此外,及时、恰当且明智选择的治疗(介入或手术)可带来顺利的治疗和康复。