Department of Public Health and Primary Care, KU Leuven, Leuven, Belgium.
Test Evaluation Research Group, Institute of Applied Health Research, University of Birmingham, Birmingham, UK.
Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3.
COVID-19 illness is highly variable, ranging from infection with no symptoms through to pneumonia and life-threatening consequences. Symptoms such as fever, cough, or loss of sense of smell (anosmia) or taste (ageusia), can help flag early on if the disease is present. Such information could be used either to rule out COVID-19 disease, or to identify people who need to go for COVID-19 diagnostic tests. This is the second update of this review, which was first published in 2020.
To assess the diagnostic accuracy of signs and symptoms to determine if a person presenting in primary care or to hospital outpatient settings, such as the emergency department or dedicated COVID-19 clinics, has COVID-19.
We undertook electronic searches up to 10 June 2021 in the University of Bern living search database. In addition, we checked repositories of COVID-19 publications. We used artificial intelligence text analysis to conduct an initial classification of documents. We did not apply any language restrictions.
Studies were eligible if they included people with clinically suspected COVID-19, or recruited known cases with COVID-19 and also controls without COVID-19 from a single-gate cohort. Studies were eligible when they recruited people presenting to primary care or hospital outpatient settings. Studies that included people who contracted SARS-CoV-2 infection while admitted to hospital were not eligible. The minimum eligible sample size of studies was 10 participants. All signs and symptoms were eligible for this review, including individual signs and symptoms or combinations. We accepted a range of reference standards.
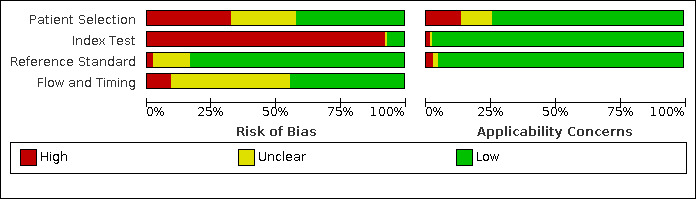
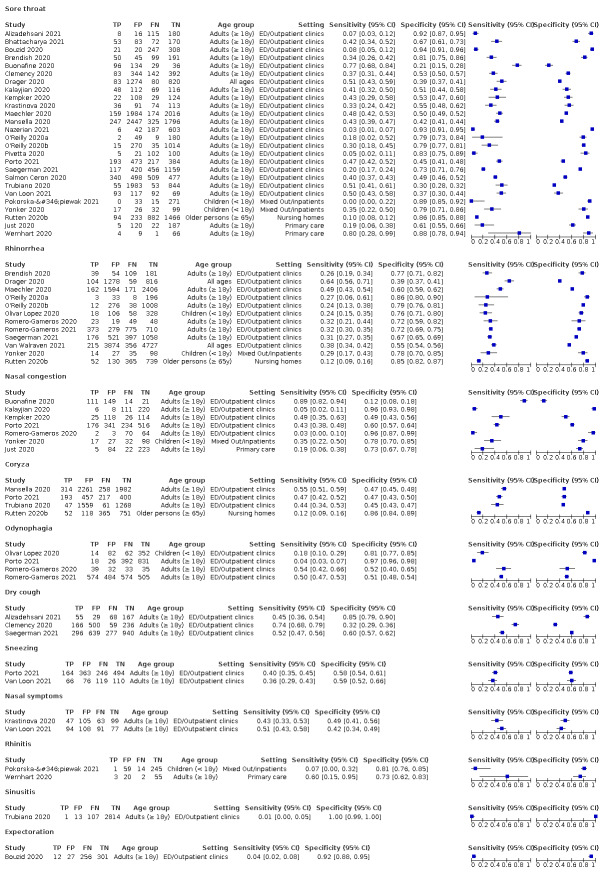
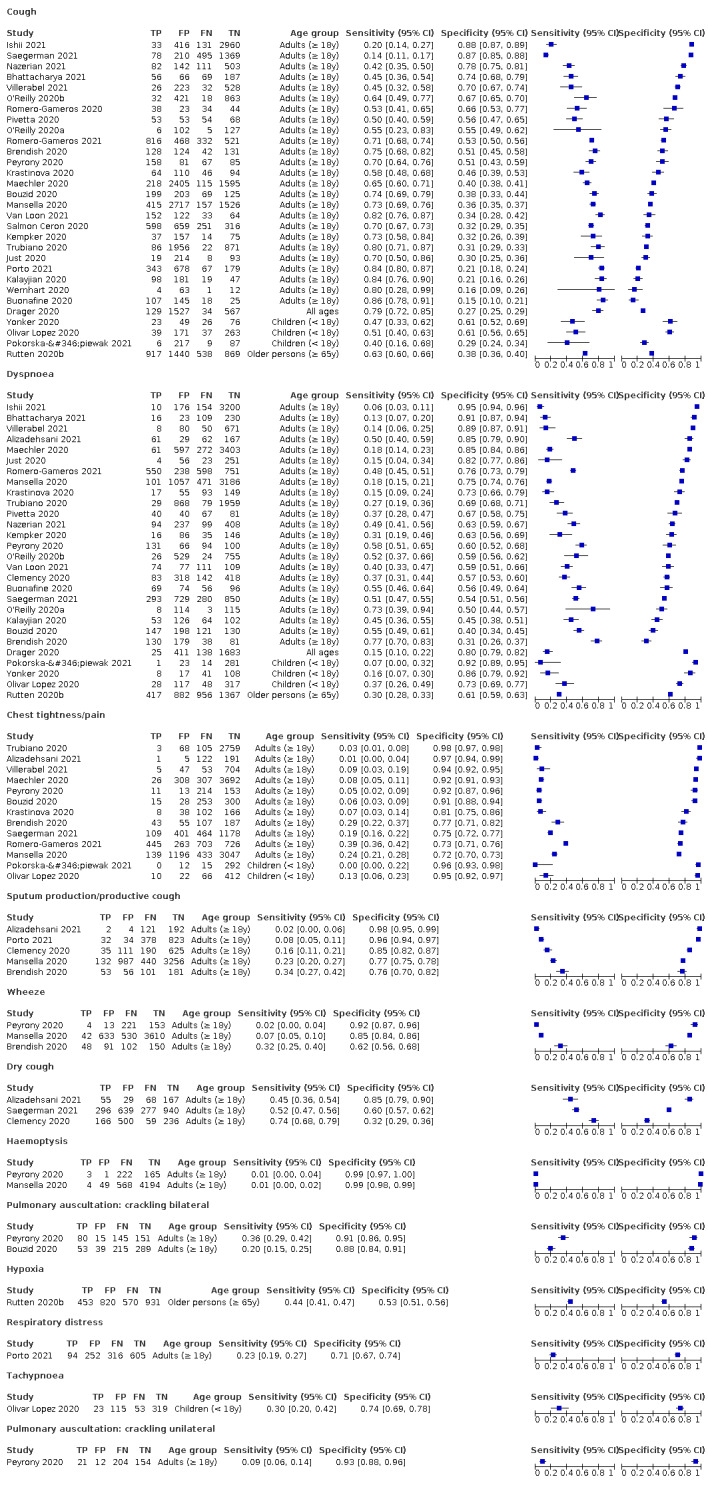
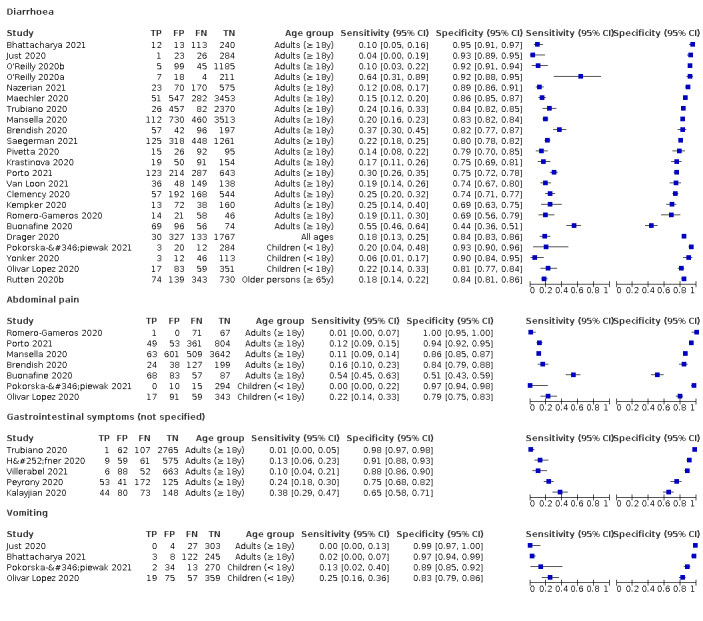
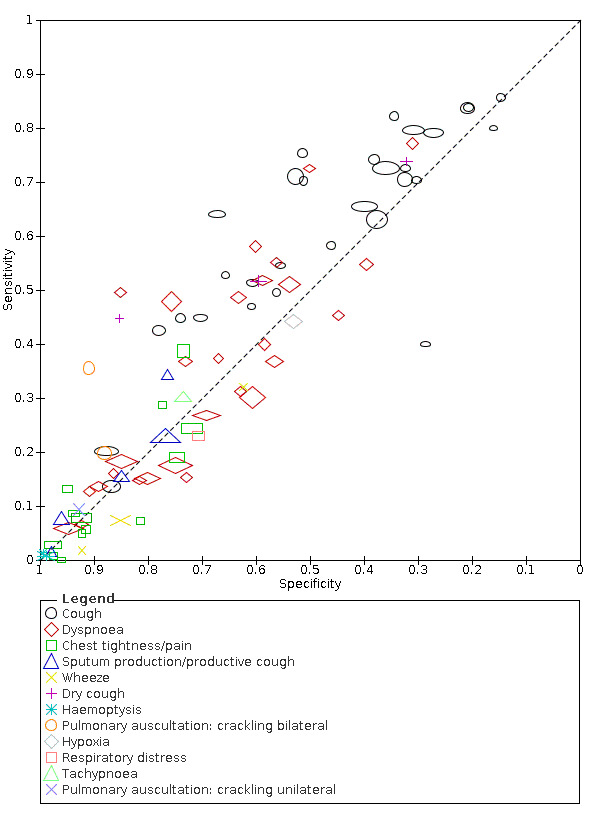
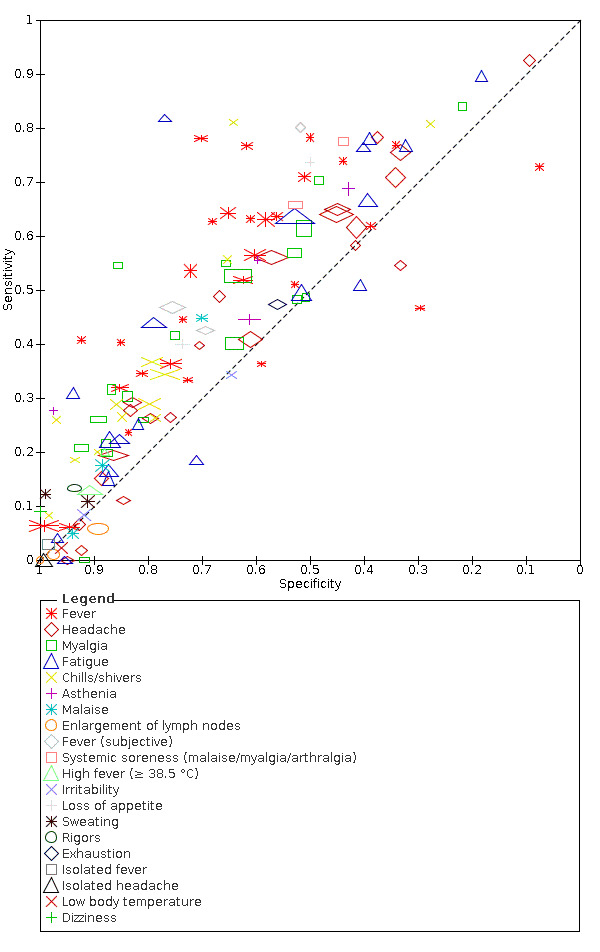
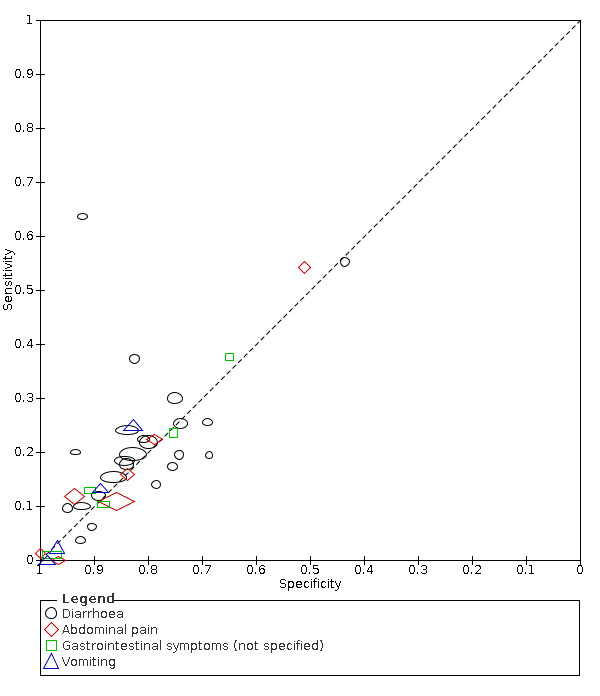
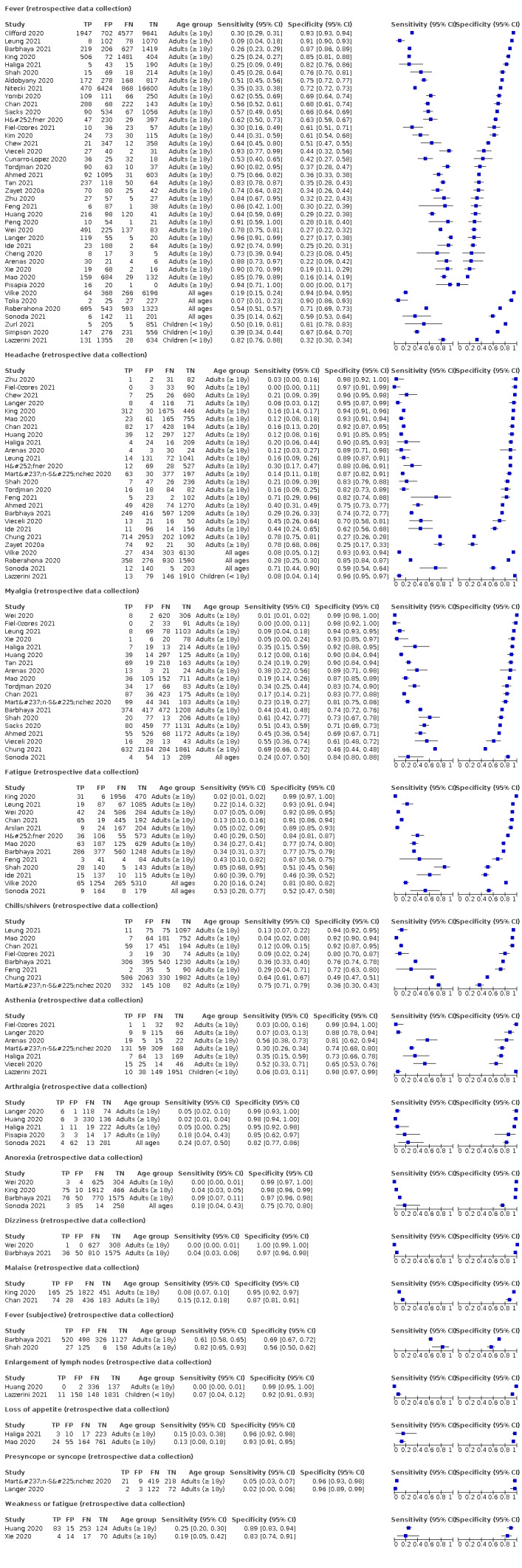
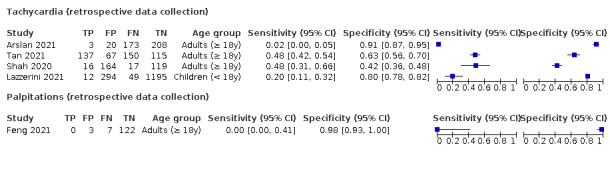
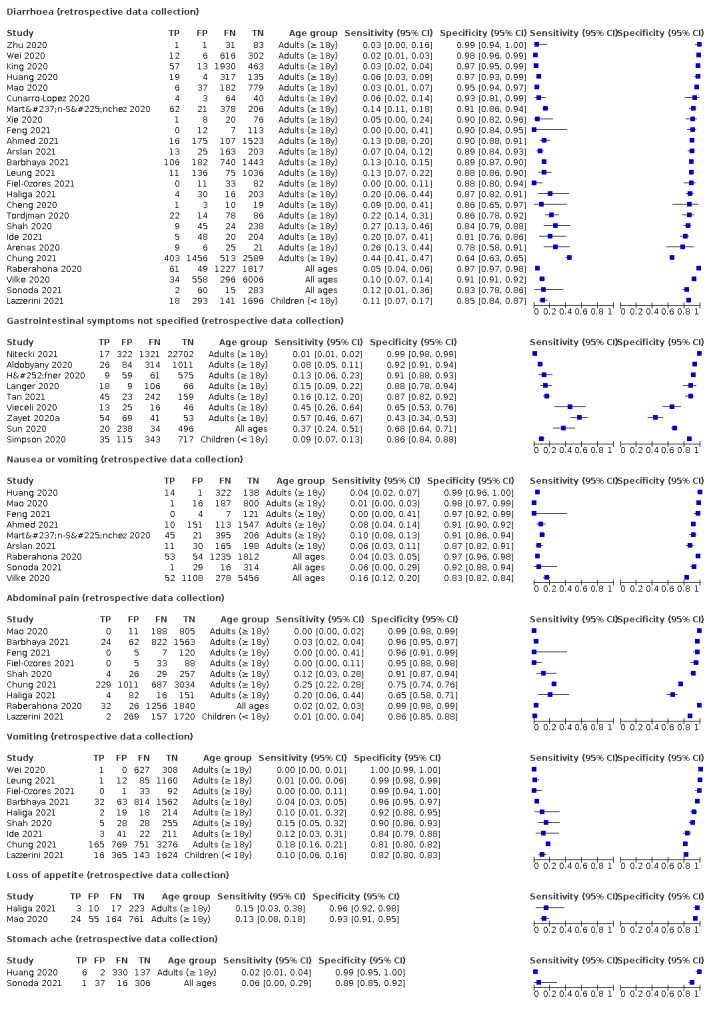
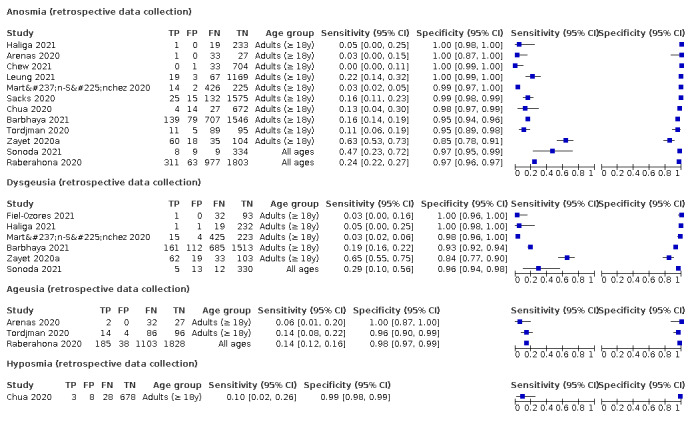
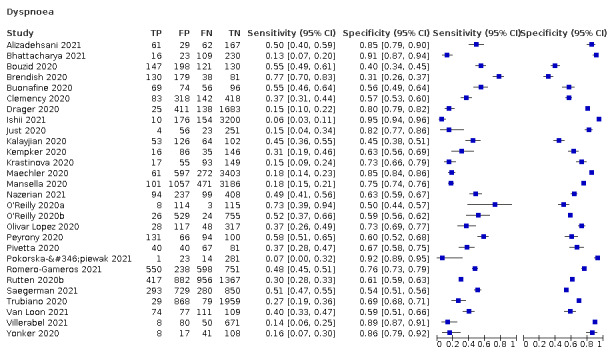
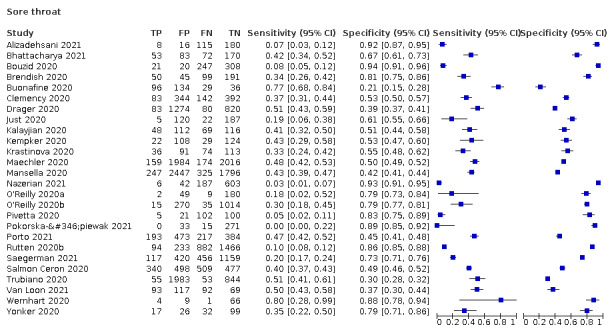
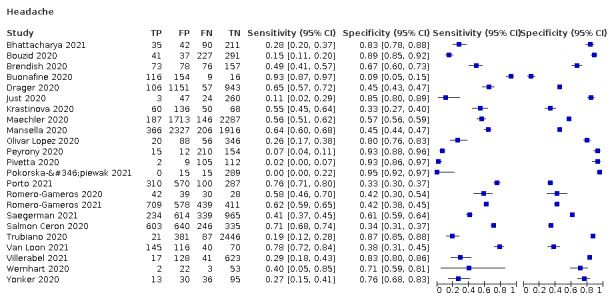
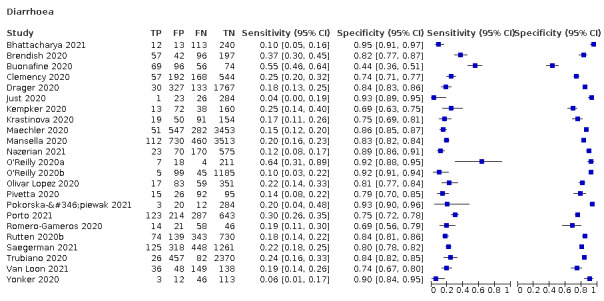
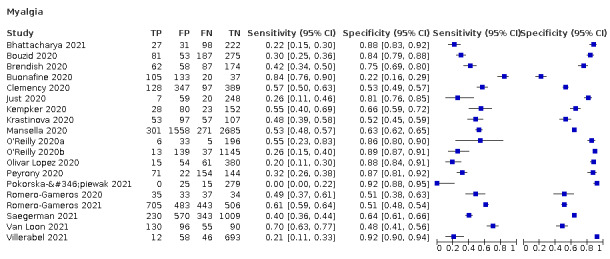
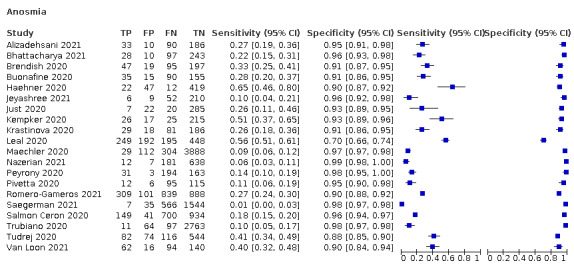
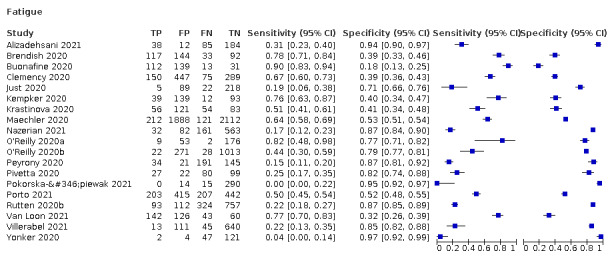
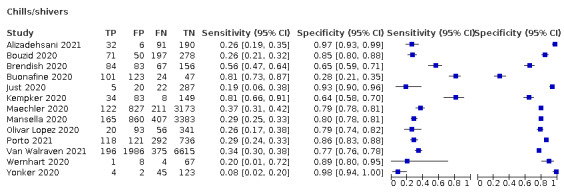
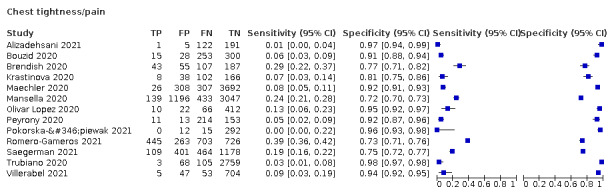
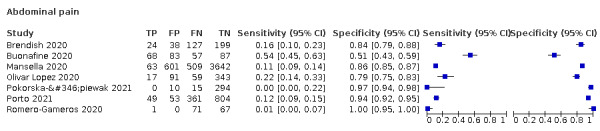
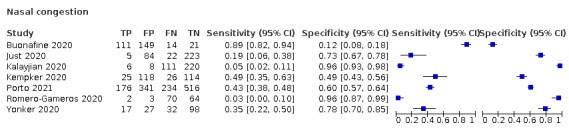
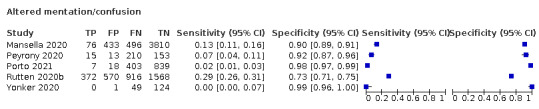
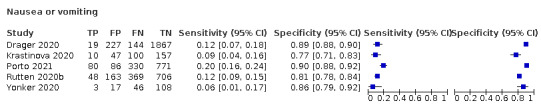
Pairs of review authors independently selected all studies, at both title and abstract, and full-text stage. They resolved any disagreements by discussion with a third review author. Two review authors independently extracted data and assessed risk of bias using the QUADAS-2 checklist, and resolved disagreements by discussion with a third review author. Analyses were restricted to prospective studies only. We presented sensitivity and specificity in paired forest plots, in receiver operating characteristic (ROC) space and in dumbbell plots. We estimated summary parameters using a bivariate random-effects meta-analysis whenever five or more primary prospective studies were available, and whenever heterogeneity across studies was deemed acceptable.
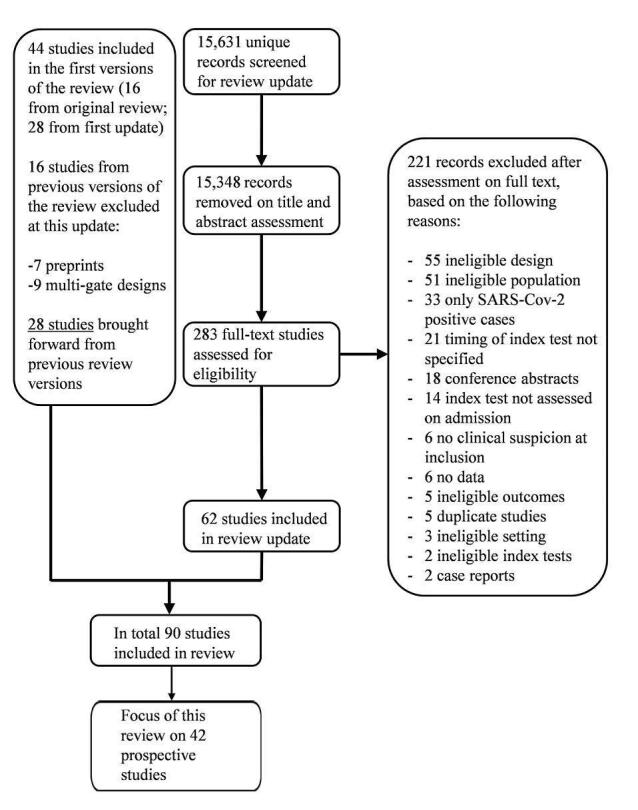
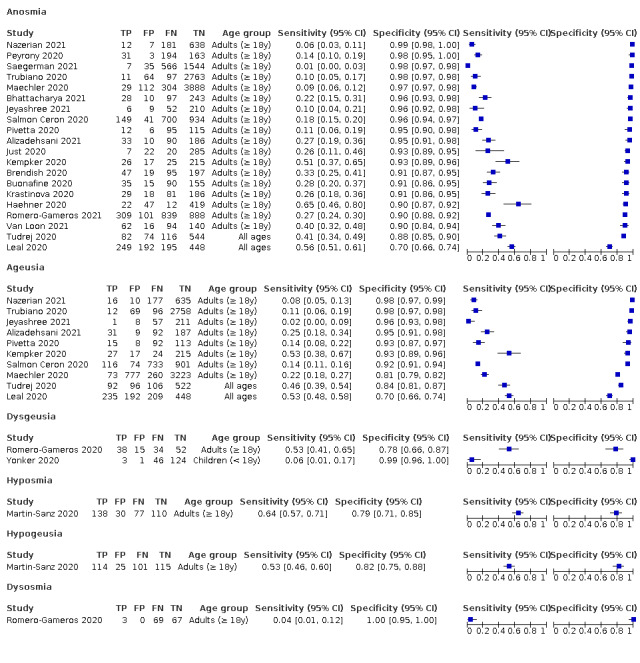
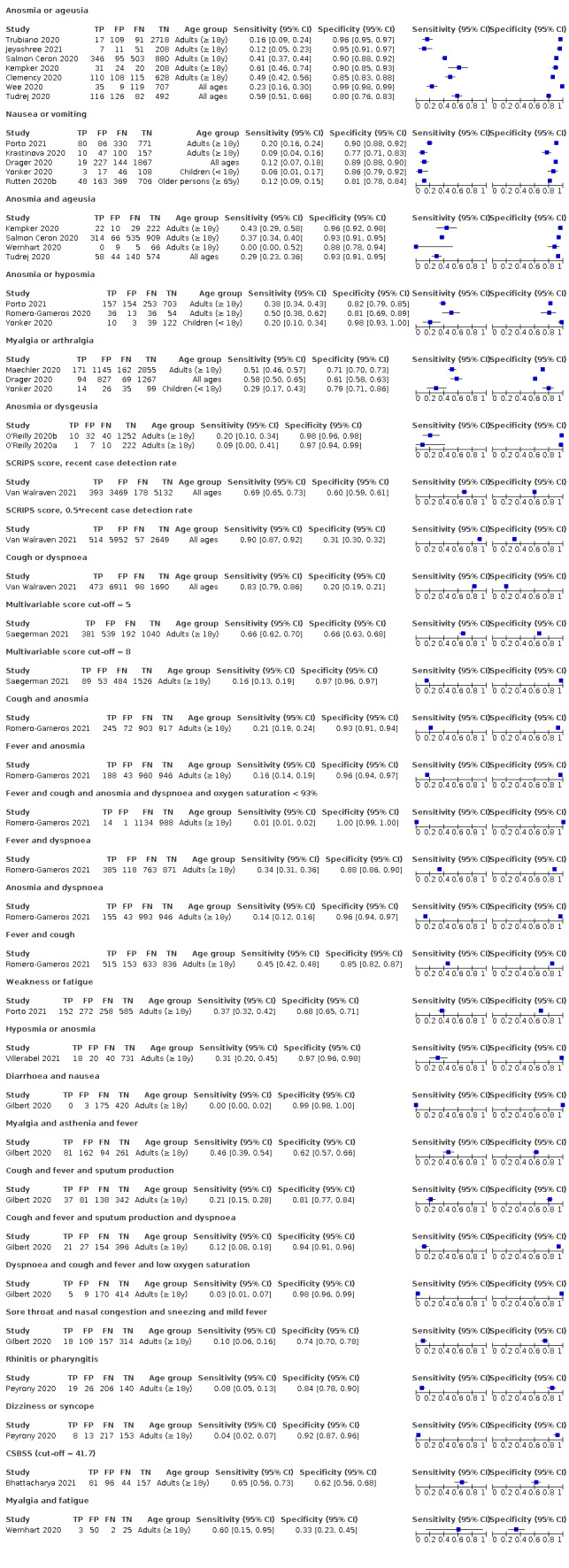
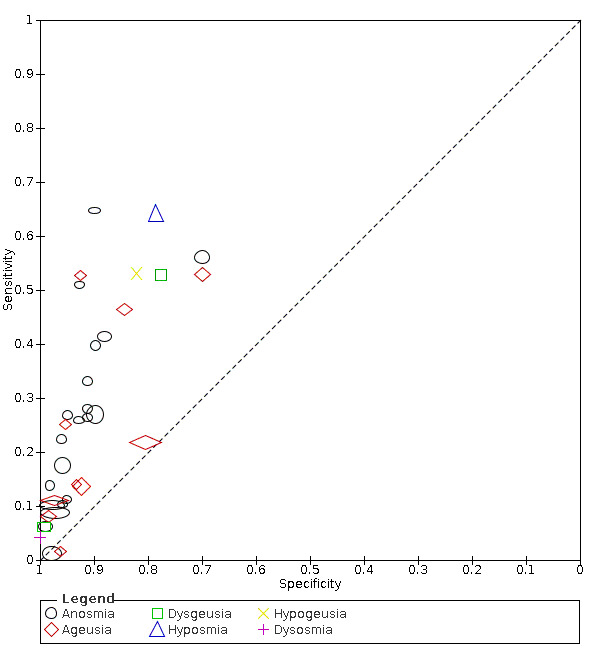
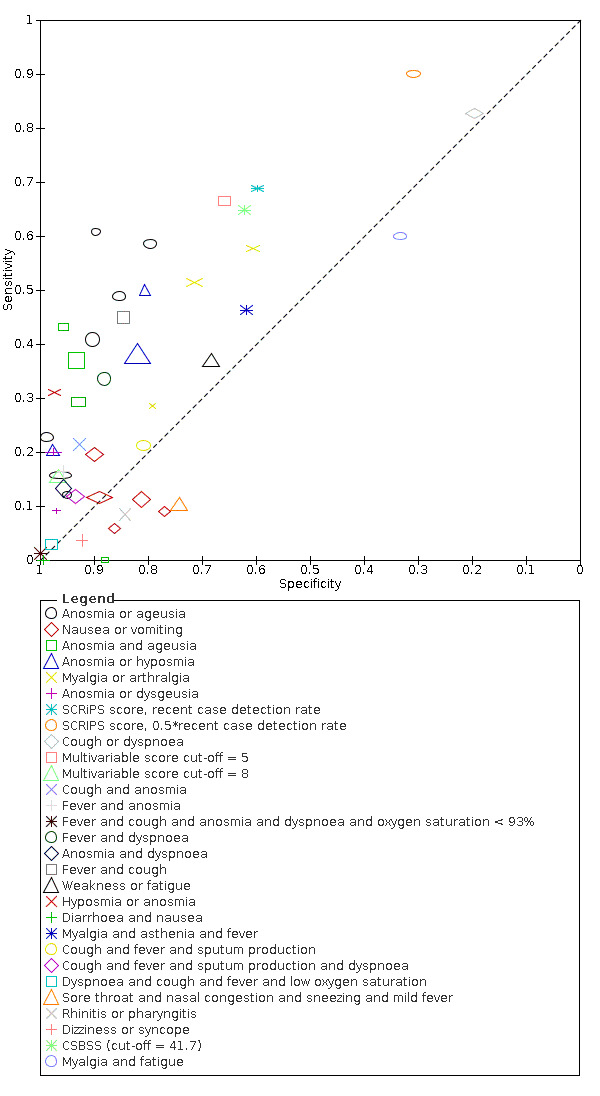
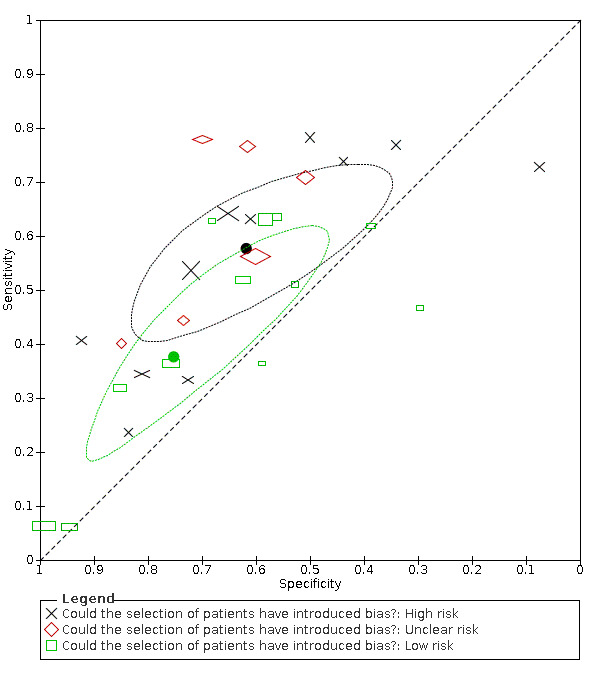
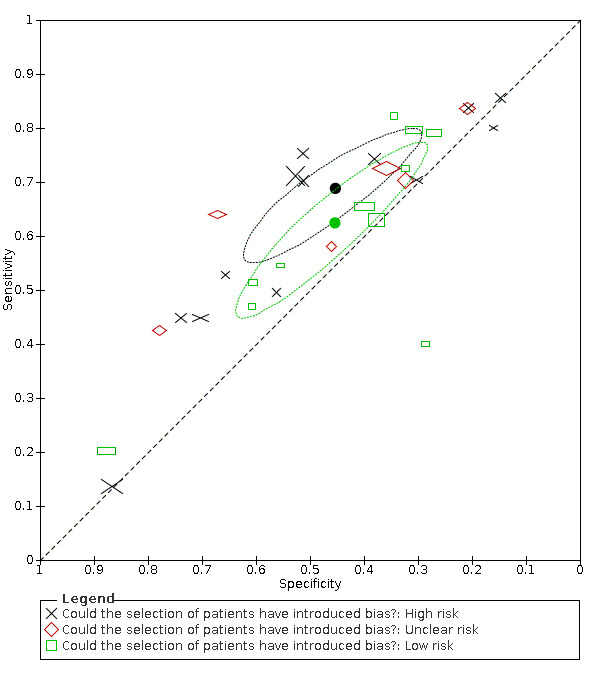
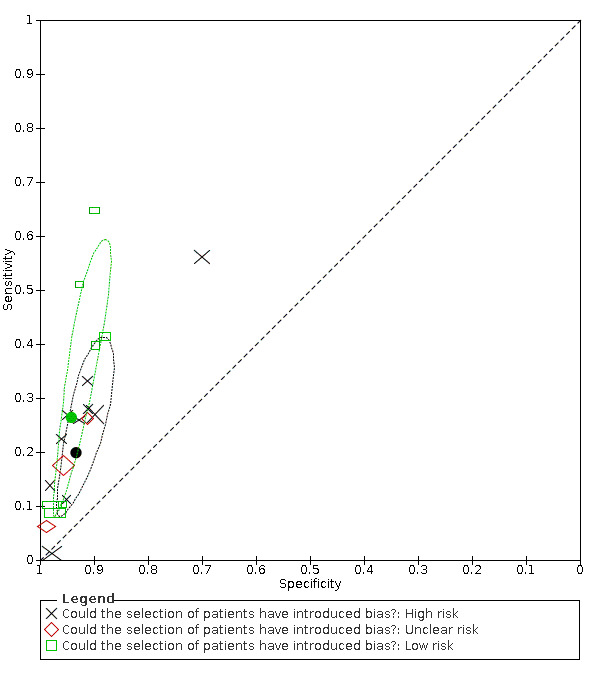
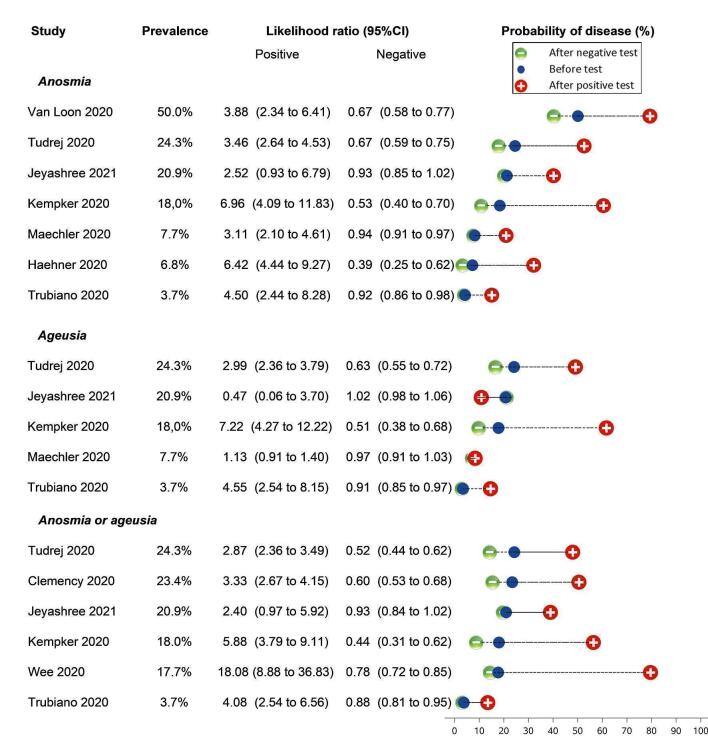
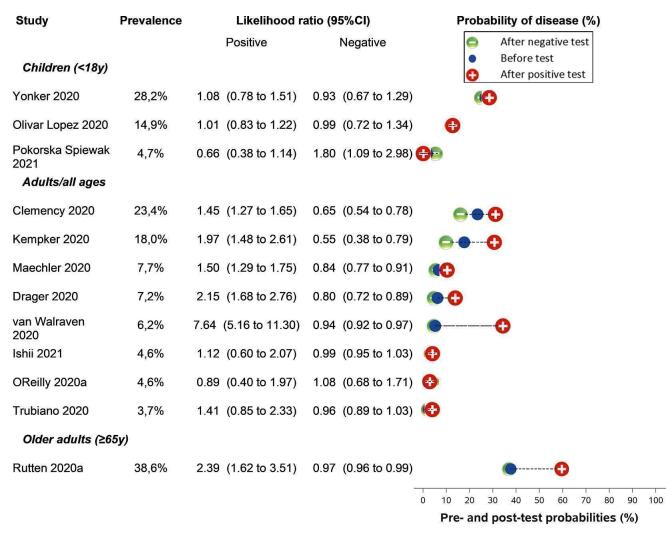
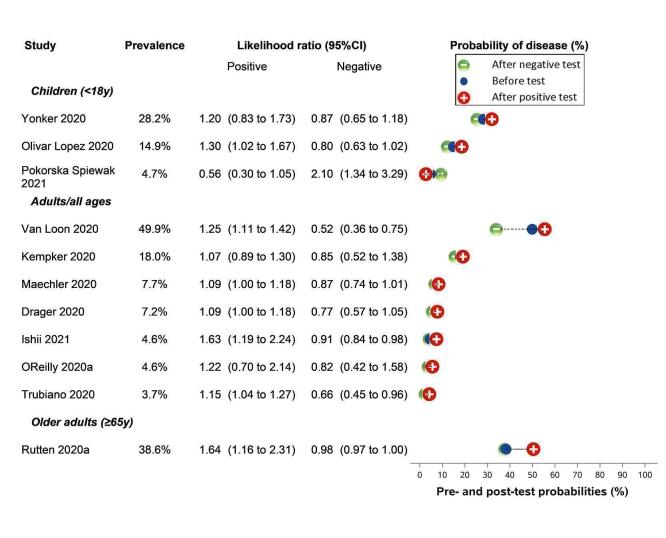
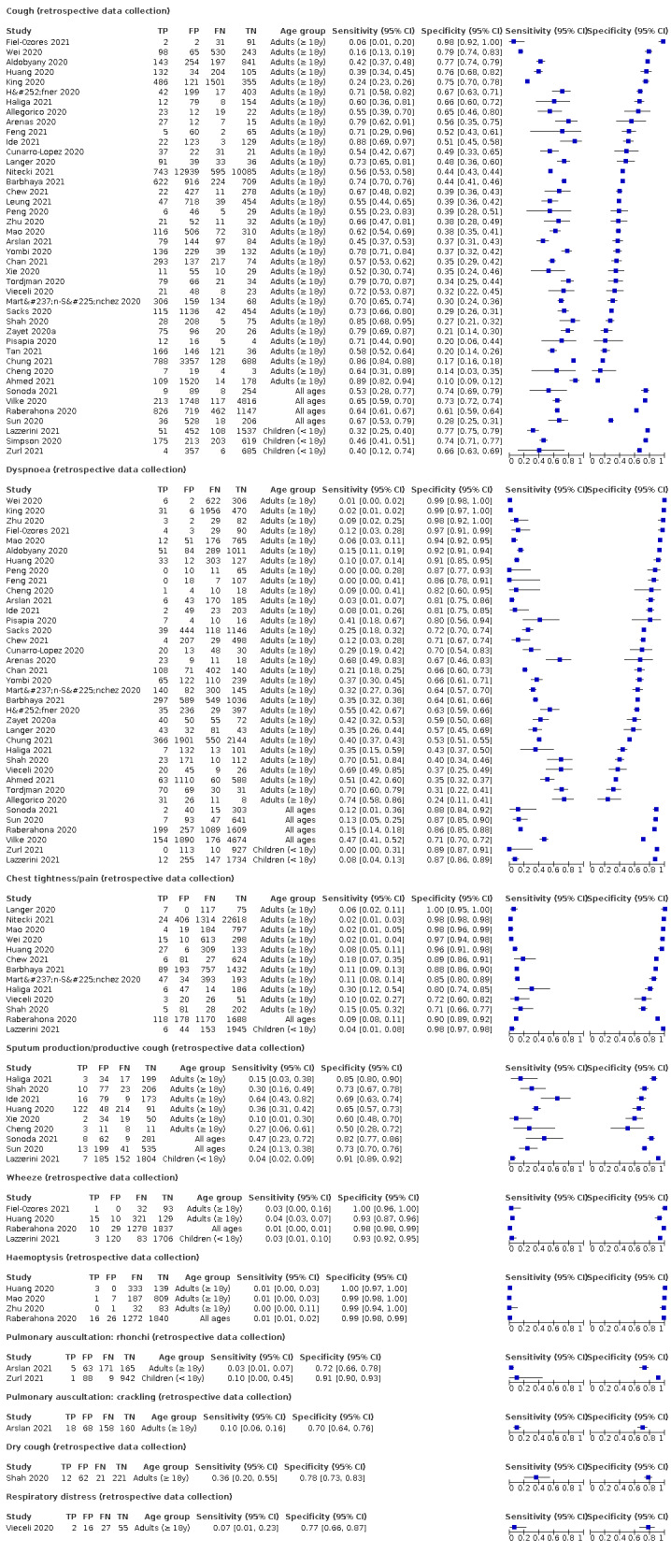
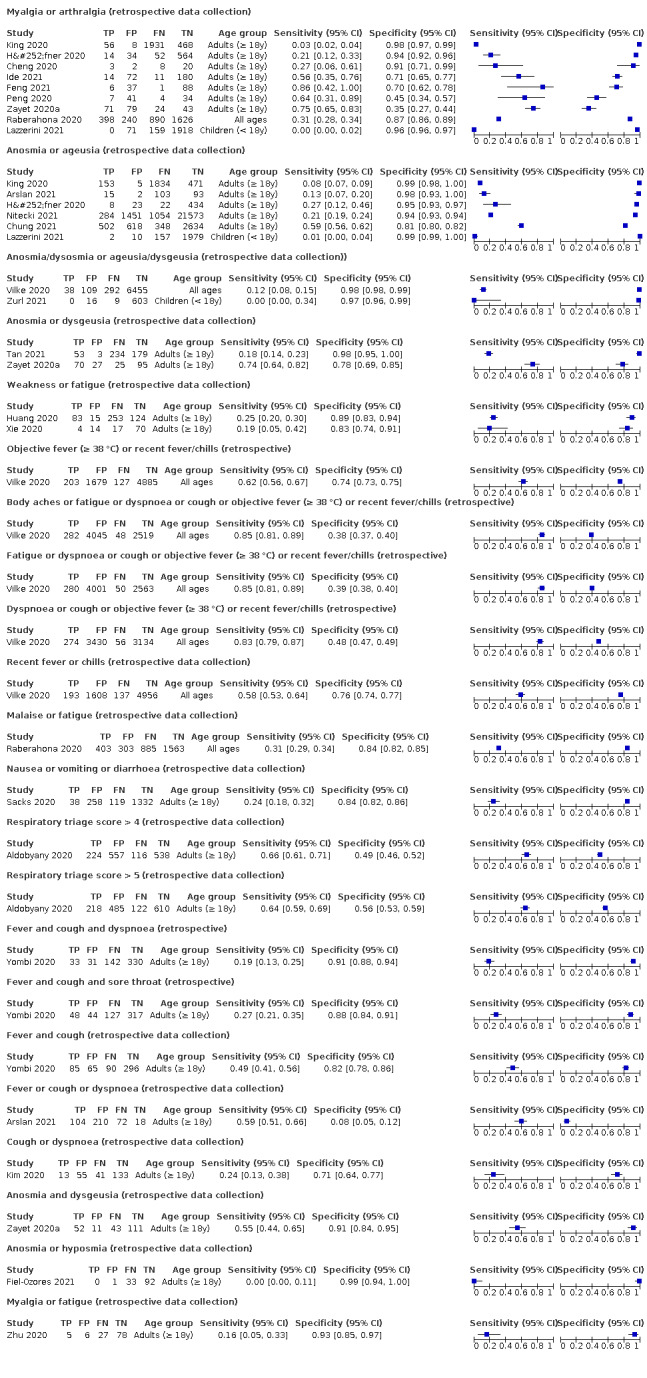
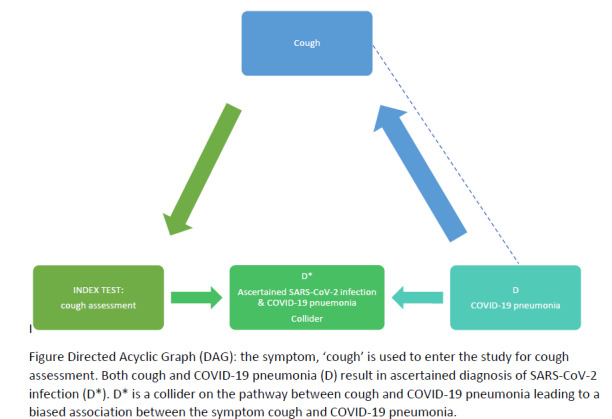
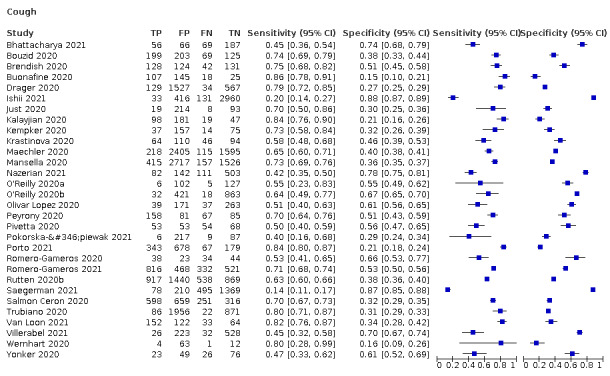
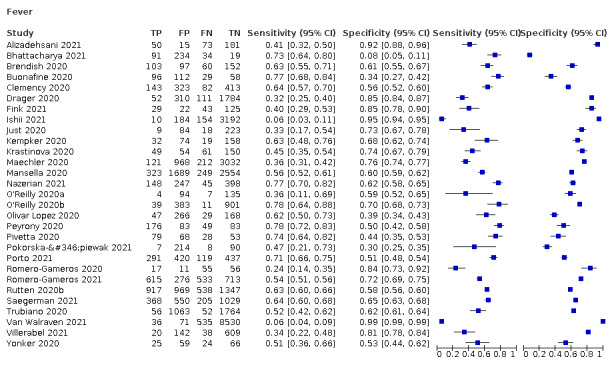
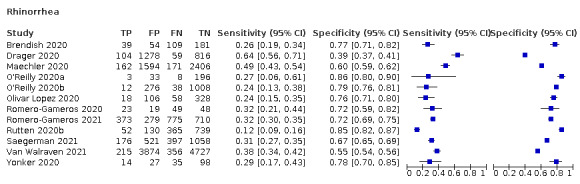
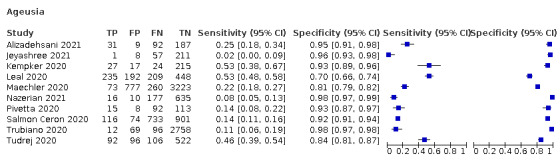
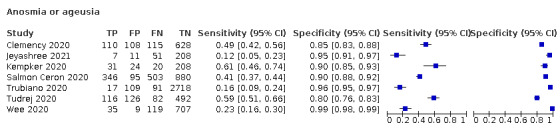
We identified 90 studies; for this update we focused on the results of 42 prospective studies with 52,608 participants. Prevalence of COVID-19 disease varied from 3.7% to 60.6% with a median of 27.4%. Thirty-five studies were set in emergency departments or outpatient test centres (46,878 participants), three in primary care settings (1230 participants), two in a mixed population of in- and outpatients in a paediatric hospital setting (493 participants), and two overlapping studies in nursing homes (4007 participants). The studies did not clearly distinguish mild COVID-19 disease from COVID-19 pneumonia, so we present the results for both conditions together. Twelve studies had a high risk of bias for selection of participants because they used a high level of preselection to decide whether reverse transcription polymerase chain reaction (RT-PCR) testing was needed, or because they enrolled a non-consecutive sample, or because they excluded individuals while they were part of the study base. We rated 36 of the 42 studies as high risk of bias for the index tests because there was little or no detail on how, by whom and when, the symptoms were measured. For most studies, eligibility for testing was dependent on the local case definition and testing criteria that were in effect at the time of the study, meaning most people who were included in studies had already been referred to health services based on the symptoms that we are evaluating in this review. The applicability of the results of this review iteration improved in comparison with the previous reviews. This version has more studies of people presenting to ambulatory settings, which is where the majority of assessments for COVID-19 take place. Only three studies presented any data on children separately, and only one focused specifically on older adults. We found data on 96 symptoms or combinations of signs and symptoms. Evidence on individual signs as diagnostic tests was rarely reported, so this review reports mainly on the diagnostic value of symptoms. Results were highly variable across studies. Most had very low sensitivity and high specificity. RT-PCR was the most often used reference standard (40/42 studies). Only cough (11 studies) had a summary sensitivity above 50% (62.4%, 95% CI 50.6% to 72.9%)); its specificity was low (45.4%, 95% CI 33.5% to 57.9%)). Presence of fever had a sensitivity of 37.6% (95% CI 23.4% to 54.3%) and a specificity of 75.2% (95% CI 56.3% to 87.8%). The summary positive likelihood ratio of cough was 1.14 (95% CI 1.04 to 1.25) and that of fever 1.52 (95% CI 1.10 to 2.10). Sore throat had a summary positive likelihood ratio of 0.814 (95% CI 0.714 to 0.929), which means that its presence increases the probability of having an infectious disease other than COVID-19. Dyspnoea (12 studies) and fatigue (8 studies) had a sensitivity of 23.3% (95% CI 16.4% to 31.9%) and 40.2% (95% CI 19.4% to 65.1%) respectively. Their specificity was 75.7% (95% CI 65.2% to 83.9%) and 73.6% (95% CI 48.4% to 89.3%). The summary positive likelihood ratio of dyspnoea was 0.96 (95% CI 0.83 to 1.11) and that of fatigue 1.52 (95% CI 1.21 to 1.91), which means that the presence of fatigue slightly increases the probability of having COVID-19. Anosmia alone (7 studies), ageusia alone (5 studies), and anosmia or ageusia (6 studies) had summary sensitivities below 50% but summary specificities over 90%. Anosmia had a summary sensitivity of 26.4% (95% CI 13.8% to 44.6%) and a specificity of 94.2% (95% CI 90.6% to 96.5%). Ageusia had a summary sensitivity of 23.2% (95% CI 10.6% to 43.3%) and a specificity of 92.6% (95% CI 83.1% to 97.0%). Anosmia or ageusia had a summary sensitivity of 39.2% (95% CI 26.5% to 53.6%) and a specificity of 92.1% (95% CI 84.5% to 96.2%). The summary positive likelihood ratios of anosmia alone and anosmia or ageusia were 4.55 (95% CI 3.46 to 5.97) and 4.99 (95% CI 3.22 to 7.75) respectively, which is just below our arbitrary definition of a 'red flag', that is, a positive likelihood ratio of at least 5. The summary positive likelihood ratio of ageusia alone was 3.14 (95% CI 1.79 to 5.51). Twenty-four studies assessed combinations of different signs and symptoms, mostly combining olfactory symptoms. By combining symptoms with other information such as contact or travel history, age, gender, and a local recent case detection rate, some multivariable prediction scores reached a sensitivity as high as 90%.
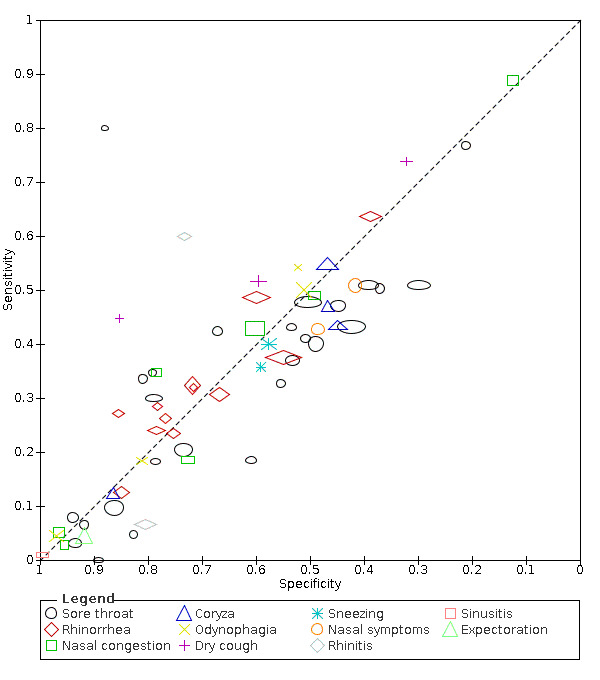
AUTHORS' CONCLUSIONS: Most individual symptoms included in this review have poor diagnostic accuracy. Neither absence nor presence of symptoms are accurate enough to rule in or rule out the disease. The presence of anosmia or ageusia may be useful as a red flag for the presence of COVID-19. The presence of cough also supports further testing. There is currently no evidence to support further testing with PCR in any individuals presenting only with upper respiratory symptoms such as sore throat, coryza or rhinorrhoea. Combinations of symptoms with other readily available information such as contact or travel history, or the local recent case detection rate may prove more useful and should be further investigated in an unselected population presenting to primary care or hospital outpatient settings. The diagnostic accuracy of symptoms for COVID-19 is moderate to low and any testing strategy using symptoms as selection mechanism will result in both large numbers of missed cases and large numbers of people requiring testing. Which one of these is minimised, is determined by the goal of COVID-19 testing strategies, that is, controlling the epidemic by isolating every possible case versus identifying those with clinically important disease so that they can be monitored or treated to optimise their prognosis. The former will require a testing strategy that uses very few symptoms as entry criterion for testing, the latter could focus on more specific symptoms such as fever and anosmia.
COVID-19 疾病的表现差异很大,从无症状感染到肺炎和危及生命的后果不等。发烧、咳嗽或嗅觉(嗅觉丧失)或味觉(味觉丧失)等症状可以帮助早期发现疾病是否存在。这些信息可用于排除 COVID-19 疾病,或识别需要进行 COVID-19 诊断检测的人。这是对首次发表于 2020 年的该综述的第二次更新。
评估体征和症状的诊断准确性,以确定在初级保健或医院门诊环境(如急诊科或专门的 COVID-19 诊所)就诊的患者是否患有 COVID-19。
我们于 2021 年 6 月 10 日在伯尔尼大学生活搜索数据库中进行了电子检索。此外,我们还检查了 COVID-19 出版物的存储库。我们使用人工智能文本分析对文件进行了初步分类。我们没有对语言进行任何限制。
如果研究包括临床上疑似 COVID-19 的患者,或招募了已知 COVID-19 病例和来自单一门急诊队列的对照患者,则研究符合纳入标准。如果研究招募了因其他原因住院但后来被确诊为 COVID-19 的患者,则研究不符合纳入标准。纳入研究的最低合格样本量为 10 名参与者。本综述纳入了所有体征和症状,包括单个体征和症状或组合。我们接受了一系列参考标准。
两名综述作者分别独立地在标题和摘要以及全文阶段对所有研究进行了选择。任何有争议的问题都通过与第三名综述作者讨论来解决。两名综述作者独立提取数据,并使用 QUADAS-2 清单评估风险偏倚,任何有争议的问题都通过与第三名综述作者讨论来解决。分析仅限于前瞻性研究。我们以配对森林图、接收器操作特征(ROC)空间和哑铃图展示了敏感性和特异性。只要有五个或更多的主要前瞻性研究,并且研究之间的异质性被认为是可以接受的,我们就使用二变量随机效应荟萃分析来估计汇总参数。
我们确定了 90 项研究;本次更新主要关注的是 42 项前瞻性研究,涉及 52608 名参与者。COVID-19 疾病的患病率为 3.7%至 60.6%,中位数为 27.4%。35 项研究是在急诊科或门诊检测中心进行的(46878 名参与者),3 项是在初级保健环境中进行的(1230 名参与者),2 项是在儿科医院混合门诊和住院患者环境中进行的(493 名参与者),2 项重叠研究是在养老院进行的(4007 名参与者)。这些研究没有明确区分轻度 COVID-19 疾病和 COVID-19 肺炎,因此我们将这两种情况的结果一起呈现。12 项研究由于使用了较高的预先筛选水平来决定是否需要进行 RT-PCR 检测,或由于招募的是非连续样本,或由于在研究期间将参与者排除在外,因此存在较高的选择参与者偏倚风险。我们认为 42 项研究中的 36 项在测量症状时存在较高的指数试验偏倚风险,因为很少或没有详细说明如何、由谁以及何时测量症状。对于大多数研究,检测的资格取决于当地的病例定义和检测标准,这些标准是在研究进行时生效的,这意味着大多数被纳入研究的人已经根据本综述中评估的症状被转诊到卫生服务机构。与前几次综述相比,本研究的适用性有所提高。本次迭代版本有更多的研究对象来自门诊环境,这是大多数 COVID-19 评估发生的地方。只有三项研究分别单独报告了儿童数据,只有一项专门针对老年人。我们共报告了 96 个症状或体征和症状组合。很少有研究报告单个症状作为诊断试验的证据,因此本综述主要报告症状的诊断价值。结果在研究之间差异很大。大多数研究的敏感性很低,特异性很高。RT-PCR 是最常使用的参考标准(40/42 项研究)。只有咳嗽(11 项研究)的敏感性超过 50%(62.4%,95%CI 50.6%至 72.9%));特异性较低(45.4%,95%CI 33.5%至 57.9%)。发热的敏感性为 37.6%(95%CI 23.4%至 54.3%),特异性为 75.2%(95%CI 56.3%至 87.8%)。咳嗽的阳性似然比为 1.14(95%CI 1.04 至 1.25),发热的阳性似然比为 1.52(95%CI 1.10 至 2.10)。咽痛的阳性似然比为 0.814(95%CI 0.714 至 0.929),这意味着其存在增加了患有除 COVID-19 以外的传染病的可能性。呼吸困难(12 项研究)和疲劳(8 项研究)的敏感性分别为 23.3%(95%CI 16.4%至 31.9%)和 40.2%(95%CI 19.4%至 65.1%)。它们的特异性分别为 75.7%(95%CI 65.2%至 83.9%)和 73.6%(95%CI 48.4%至 89.3%)。呼吸困难的阳性似然比为 0.96(95%CI 0.83 至 1.11),疲劳的阳性似然比为 1.52(95%CI 1.21 至 1.91),这意味着疲劳的存在略微增加了患有 COVID-19 的可能性。单独嗅觉丧失(7 项研究)、单独味觉丧失(5 项研究)以及嗅觉丧失或味觉丧失(6 项研究)的敏感性均低于 50%,但特异性均高于 90%。嗅觉丧失的敏感性为 26.4%(95%CI 13.8%至 44.6%),特异性为 94.2%(95%CI 90.6%至 96.5%)。味觉丧失的敏感性为 23.2%(95%CI 10.6%至 43.3%),特异性为 92.6%(95%CI 83.1%至 97.0%)。嗅觉丧失或味觉丧失的敏感性为 39.2%(95%CI 26.5%至 53.6%),特异性为 92.1%(95%CI 84.5%至 96.2%)。嗅觉丧失单独和嗅觉丧失或味觉丧失的阳性似然比分别为 4.55(95%CI 3.46 至 5.97)和 4.99(95%CI 3.22 至 7.75),接近我们定义的“红色标记”,即阳性似然比至少为 5。味觉丧失单独的阳性似然比为 3.14(95%CI 1.79 至 5.51)。24 项研究评估了不同症状组合,主要是嗅觉症状的组合。通过将症状与其他信息(如接触史或旅行史、年龄、性别和当地近期检出率)结合起来,一些多变量预测评分的敏感性高达 90%。
大多数纳入本综述的单个症状的诊断准确性较差。没有任何单一症状的存在或不存在足以排除或诊断 COVID-19 疾病。嗅觉丧失或味觉丧失可能有助于提示 COVID-19 的存在。发热也支持进一步检测。目前没有证据支持对任何仅表现为上呼吸道症状(如咽痛、鼻塞或流涕)的患者进行 PCR 进一步检测。将症状与其他容易获得的信息(如接触史或旅行史、或当地近期检出率)结合起来,可能会更有用,并应在来自初级保健或医院门诊环境的未选择人群中进一步研究。症状对 COVID-19 的诊断准确性为中度至低度,任何使用症状作为选择机制的检测策略都将导致错过大量病例和需要检测的人数增加。哪一种情况的人数减少,取决于 COVID-19 检测策略的目标,即通过隔离每一个可能