Le Saux Olivia, Sabatier Renaud, Treilleux Isabelle, Renaud Léa-Isabelle, Brachet Pierre-Emmanuel, Martinez Alejandra, Frenel Jean-Sébastien, Abdeddaim Cyril, Berthet Justine, Barrin Sarah, Colombe-Vermorel Amélie, Odeyer Laetitia, Lainé Alexandra, Caux Christophe, Dubois Bertrand, Ray-Coquard Isabelle
Cancer Research Center of Lyon, Université de Lyon, Université Claude Bernard Lyon 1, INSERM 1052, CNRS 5286, Centre Léon Bérard, "Cancer Immune Surveillance and Therapeutic Targeting" Team, 28 rue Laennec, Lyon 69008, France.
National Investigators Group for Ovarian and Breast Cancer Studies, GINEGEPS, Paris, France Department of Medical Oncology, Centre Léon Bérard, Lyon, France.
Ther Adv Med Oncol. 2025 Aug 8;17:17588359251347364. doi: 10.1177/17588359251347364. eCollection 2025.
Immune checkpoint inhibitors (ICIs) have shown efficacy in endometrial cancer (EC); however, their efficacy varies according to mismatch repair (MMR) status. Notably, even among patients with MMR-deficient (MMRd) or microsatellite instability-high (MSI-H) tumors, approximately one-third exhibit primary resistance to ICI monotherapy.
We aimed to characterize dissimilarities in the tumor immune microenvironment of ICI-treated MMRd/MSI-H versus MMR-proficient (MMRp)/microsatellite stable (MSS) EC, and to identify mechanisms of resistance.
Adults with histologically confirmed advanced or recurrent EC treated with ICIs in 6 French comprehensive cancer centers were included. Patients without available archival formalin-fixed paraffin-embedded primary tumor samples were excluded. Clinical data were collected retrospectively.
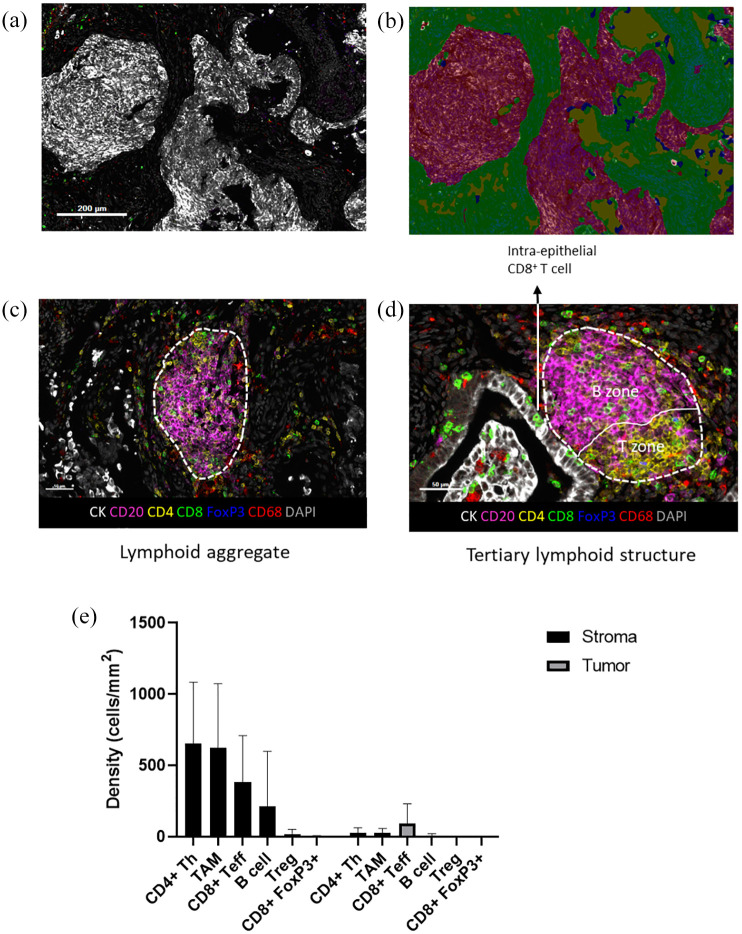
Patients were classified as ICI-Responders or Non-Responders based on best objective response. A seven-color multi-immunofluorescence staining (CD20, CD4, CD8, FoxP3, CD68, CK, and DAPI) was performed on sections from archival formalin-fixed paraffin-embedded primary tumors. Cell densities and spatial proximity were analyzed using inForm software. T/B lymphoid aggregates (LA) and tertiary lymphoid structures (TLS) were separately quantified. Microsatellite status, presence of LA/TLS, and immune cell densities were correlated to response to treatment.
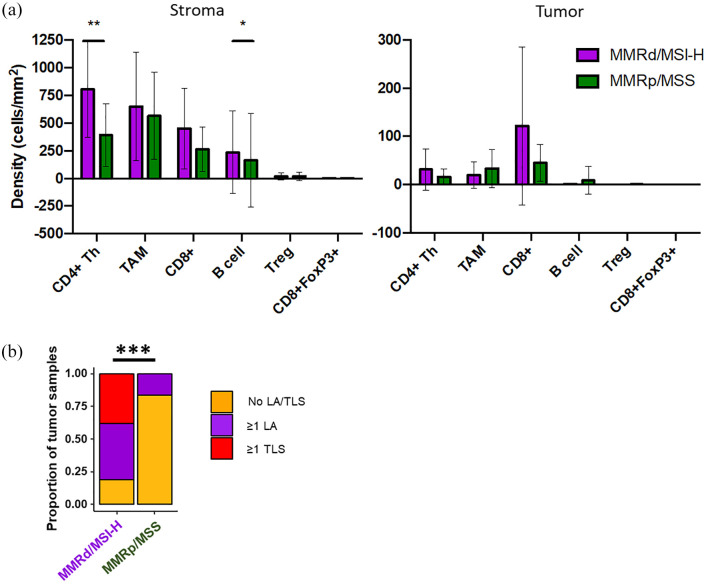
Twenty-one MMRd/MSI-H and 12 MMRp/MSS tumors were analyzed. We observed more MMRd/MSI-H tumors with LA/TLS compared to MMRp/MSS cases: 81% versus 17%, ⩽ 0.001. There were more CD8 T effector cells in the vicinity of B cells in MMRd/MSI-H tumors compared to MMRp/MSS tumors (1.26 (0-3.40) vs 0.49 (0-1.86), = 0.017), suggesting cooperation between CD8 T cells and B cells in MMRd/MSI-H tumors. No differences were shown in terms of the presence of LA/TLS and the subsequent response to ICI in EC ( = 0.400). Using a multivariate logistic regression model, we found that a low density of CD68 tumor-associated macrophages (TAMs) in the stroma, was associated with response to ICI in EC (odds ratio = 11.67, 95% CI (1.69-237.45), = 0.033) and showed good accuracy in predicting response to ICI in the whole cohort (AUC = 0.75, 95% CI (0.59-0.91)).
We characterize the immune landscape in EC patients treated with ICIs. Distinct immune infiltrate patterns were observed in MMRd/MSI-H and MMRp/MSS tumors. A significant negative association between TAM density and ICI response was shown.
免疫检查点抑制剂(ICI)已在子宫内膜癌(EC)中显示出疗效;然而,其疗效因错配修复(MMR)状态而异。值得注意的是,即使在错配修复缺陷(MMRd)或微卫星高度不稳定(MSI-H)肿瘤患者中,约三分之一的患者对ICI单药治疗表现出原发性耐药。
我们旨在描述接受ICI治疗的MMRd/MSI-H与错配修复功能正常(MMRp)/微卫星稳定(MSS)的EC患者肿瘤免疫微环境的差异,并确定耐药机制。
纳入在6个法国综合癌症中心接受ICI治疗的组织学确诊为晚期或复发性EC的成人患者。排除没有可用的存档福尔马林固定石蜡包埋原发性肿瘤样本的患者。回顾性收集临床数据。
根据最佳客观反应将患者分为ICI反应者或无反应者。对存档的福尔马林固定石蜡包埋原发性肿瘤切片进行七色多重免疫荧光染色(CD20、CD4、CD8、FoxP3、CD68、CK和DAPI)。使用inForm软件分析细胞密度和空间接近度。分别对T/B淋巴细胞聚集物(LA)和三级淋巴结构(TLS)进行定量。微卫星状态、LA/TLS的存在以及免疫细胞密度与治疗反应相关。
分析了21例MMRd/MSI-H和12例MMRp/MSS肿瘤。我们观察到与MMRp/MSS病例相比,MMRd/MSI-H肿瘤中LA/TLS更多:81%对17%,P⩽0.001。与MMRp/MSS肿瘤相比,MMRd/MSI-H肿瘤中B细胞附近的CD8 T效应细胞更多(1.26(0-3.40)对0.49(0-1.86),P = 0.017),表明MMRd/MSI-H肿瘤中CD8 T细胞与B细胞之间存在协作。EC中LA/TLS的存在与随后对ICI的反应方面未显示差异(P = 0.400)。使用多变量逻辑回归模型,我们发现基质中CD68肿瘤相关巨噬细胞(TAM)密度低与EC中对ICI的反应相关(优势比=11.67,95%置信区间(1.69-237.45),P = 0.033),并且在预测整个队列中对ICI的反应方面显示出良好的准确性(曲线下面积=0.75,95%置信区间(0.59-0.91))。
我们描述了接受ICI治疗的EC患者的免疫格局。在MMRd/MSI-H和MMRp/MSS肿瘤中观察到不同的免疫浸润模式。显示TAM密度与ICI反应之间存在显著负相关。