Kilic Irfan Baki, Weberova Petra, VanDyke Derek, Sirova Milada, Kubesova Katerina, Fabilane Charina S, Mazhara Vladyslav, Liu Kathy, Behalova Katerina, Ptacek Bohumil, Rihova Blanka, Spangler Jamie B, Kovar Marek
Laboratory of Tumor Immunology, Institute of Microbiology of the Czech Academy of Sciences, Prague, Czech Republic.
Department of Chemical and Biomolecular Engineering, Johns Hopkins University, Baltimore, Maryland, USA.
J Immunother Cancer. 2025 Aug 11;13(8):e010465. doi: 10.1136/jitc-2024-010465.
Interleukin-2 (IL-2) immunotherapy can induce durable tumor remissions, but its clinical performance has been limited by significant drawbacks such as short serum half-life and high toxicity. Administration of IL-2 in complex with certain anti-IL-2 antibodies (IL-2cx) enhances circulation half-life while also selectivity directing the cytokine to particular immune cell subsets. In particular, IL-2cx has been developed that targets either cells expressing the CD25-containing high-affinity IL-2 receptor (ie, CD25-biased IL-2cx) or cells expressing the CD25-lacking intermediate-affinity IL-2 receptor (ie, CD25-blocking IL-2cx). Since regulatory T (Treg) cells primarily express the high-affinity IL-2 receptor whereas naïve effector T and natural killer cells mainly express the low-affinity IL-2 receptor, CD25-blocking IL-2cx have traditionally been considered as potential cancer therapeutics, particularly in combination with immune checkpoint inhibitors (ICIs).
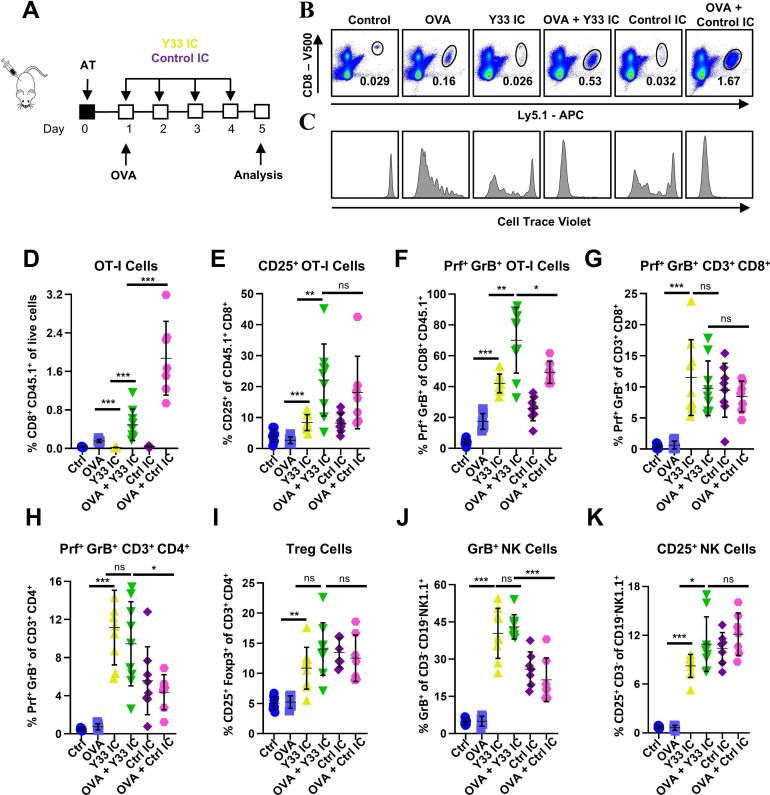
Stimulation of antigen-primed T cells by IL-2cx in the absence or presence of ICIs was evaluated through adoptive transfer of primed ovalbumin-specific T cells and analysis of expansion. Effects of IL-2cx on Treg cell-mediated inhibition of CD8 T cells were assessed by flow cytometry and thymidine incorporation. Tumor-bearing mice received combination treatments comprizing IL-2cx and ICIs, where complexes were delivered either before or after ICIs. Tumor growth and mouse survival were monitored, and immune cell phenotyping was performed. Toxicity was determined by tracking body weight, temperature, and lung edema. Substitution of IL-2cx with single-agent cytokine/antibody fusion proteins (immunocytokines, ICs) was also explored.
We showed that CD25-biased IL-2cx and ICs synergize with ICIs to completely eradicate large, established tumors despite robust Treg cell expansion. Importantly, we found that timing is crucial, as administration of IL-2cx after (but not before) ICIs led to profound antitumor effects. Mechanistically, CD25-biased IL-2cx selectively stimulated expansion and effector functions of tumor-specific CD8 T cells in a CD25-dependent manner, overcoming Treg cell-mediated suppression. Moreover, CD25-biased IL-2cx showed much lower toxicity than CD25-blocking IL-2cx, enabling a larger therapeutic window. Furthermore, we demonstrated that administration of a human IL-2-based IC significantly enhanced the antitumor activity of ICIs, establishing the translational relevance of our work.
Our findings support the temporally optimized use of CD25-biased IL-2-based therapeutics in combination with ICIs for cancer immunotherapy.
白细胞介素-2(IL-2)免疫疗法可诱导持久的肿瘤缓解,但由于血清半衰期短和毒性高等显著缺点,其临床应用受到限制。将IL-2与某些抗IL-2抗体(IL-2cx)复合给药可延长循环半衰期,同时还能将细胞因子选择性地导向特定免疫细胞亚群。特别是,已开发出靶向表达含CD25的高亲和力IL-2受体的细胞(即偏向CD25的IL-2cx)或表达缺乏CD25的中等亲和力IL-2受体的细胞(即阻断CD25的IL-2cx)的IL-2cx。由于调节性T(Treg)细胞主要表达高亲和力IL-2受体,而幼稚效应T细胞和自然杀伤细胞主要表达低亲和力IL-2受体,传统上认为阻断CD25的IL-2cx是潜在的癌症治疗药物,尤其是与免疫检查点抑制剂(ICI)联合使用时。
通过过继转移经卵清蛋白致敏的T细胞并分析其扩增情况,评估在有无ICI的情况下IL-2cx对致敏T细胞的刺激作用。通过流式细胞术和胸腺嘧啶核苷掺入法评估IL-2cx对Treg细胞介导的CD8 T细胞抑制作用的影响。荷瘤小鼠接受包含IL-2cx和ICI的联合治疗,复合物在ICI之前或之后给药。监测肿瘤生长和小鼠存活情况,并进行免疫细胞表型分析。通过跟踪体重、体温和肺水肿来确定毒性。还探索了用单药细胞因子/抗体融合蛋白(免疫细胞因子,IC)替代IL-2cx的情况。
我们发现,尽管Treg细胞大量扩增,但偏向CD25的IL-2cx和IC与ICI协同作用可完全根除已形成的大肿瘤。重要的是,我们发现给药时机至关重要,因为在ICI之后(而非之前)给予IL-2cx可产生显著的抗肿瘤效果。从机制上讲,偏向CD25的IL-2cx以CD25依赖的方式选择性刺激肿瘤特异性CD8 T细胞的扩增和效应功能,克服Treg细胞介导的抑制作用。此外,偏向CD25的IL-2cx的毒性比阻断CD25的IL-2cx低得多,从而具有更大的治疗窗口。此外,我们证明基于人IL-2的IC给药可显著增强ICI的抗肿瘤活性,确立了我们工作的转化相关性。
我们的研究结果支持在癌症免疫治疗中,将基于偏向CD25的IL-2的治疗药物与ICI进行时间上优化的联合使用。