Huang Shaoyan, Zhang Qiuwang, Wei Fujiang, Kutryk Michael J B, Zhang Jianzhong
Department of Oncology, Yantaishan Hospital Affiliated to Binzhou Medical University, Yantai, Shandong, China.
Division of Cardiology, Keenan Research Center for Biomedical Science, St. Michael's Hospital, Unity Health Toronto, University of Toronto, Toronto, ON, Canada.
Eur J Med Res. 2025 Aug 13;30(1):745. doi: 10.1186/s40001-025-03035-y.
Elevated albumin-corrected anion gap (ACAG) levels have been shown to be associated with increased mortality in various critical illnesses; however, data specifically addressing heart failure (HF) complicated by acute kidney injury (AKI) are lacking.
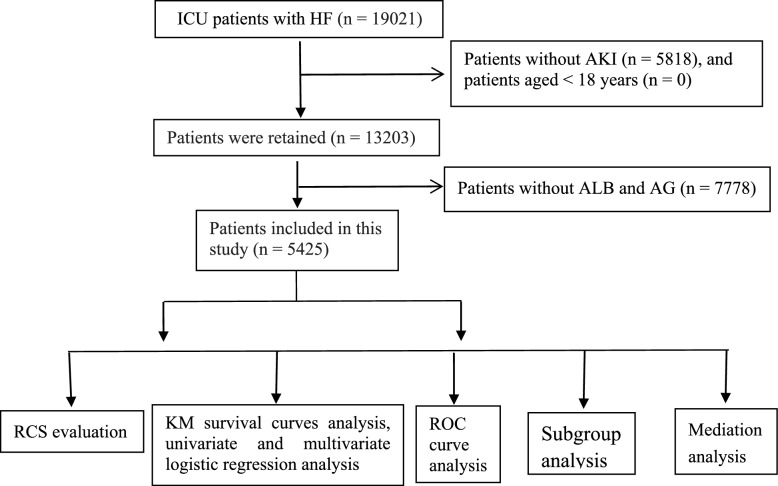
Data from ICU patients with HF complicated by AKI between 2008 and 2022 were extracted and analyzed from the MIMIC-IV database. The association between baseline ACAG levels and all-cause mortality was assessed using multiple statistical methods, including variance inflation factor analysis, restricted cubic spline (RCS) modeling, Kaplan-Meier analysis, univariate and multivariate Cox regression, subgroup analysis, mediation analysis, and receiver operating characteristic (ROC) curve analysis.
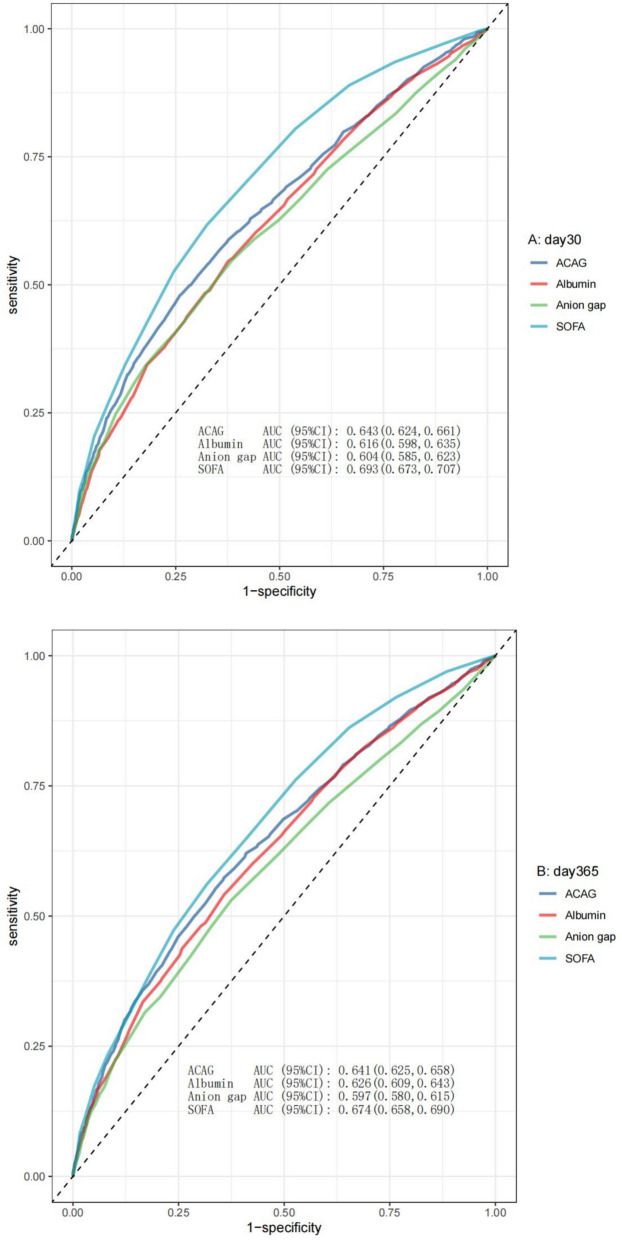
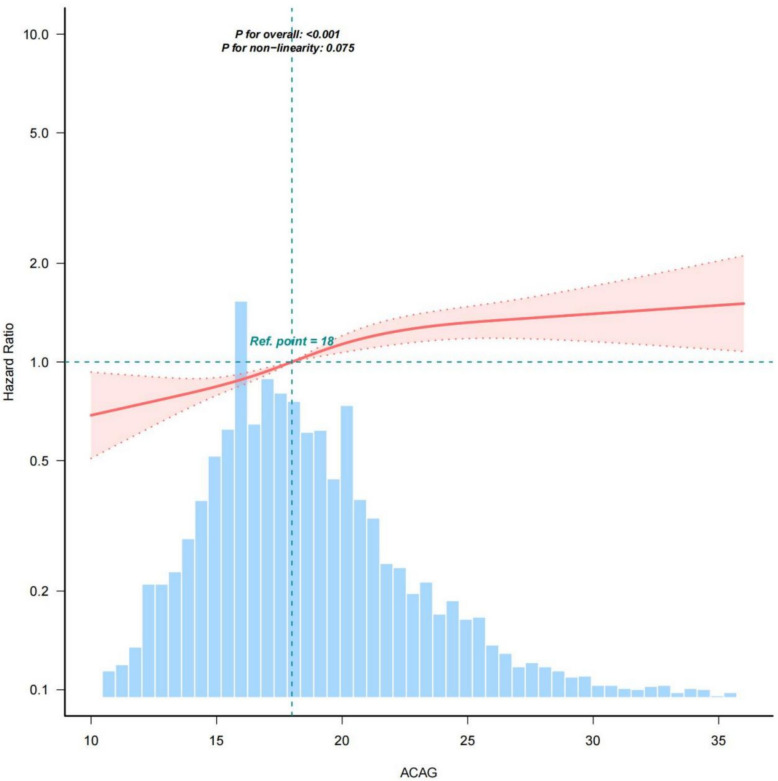
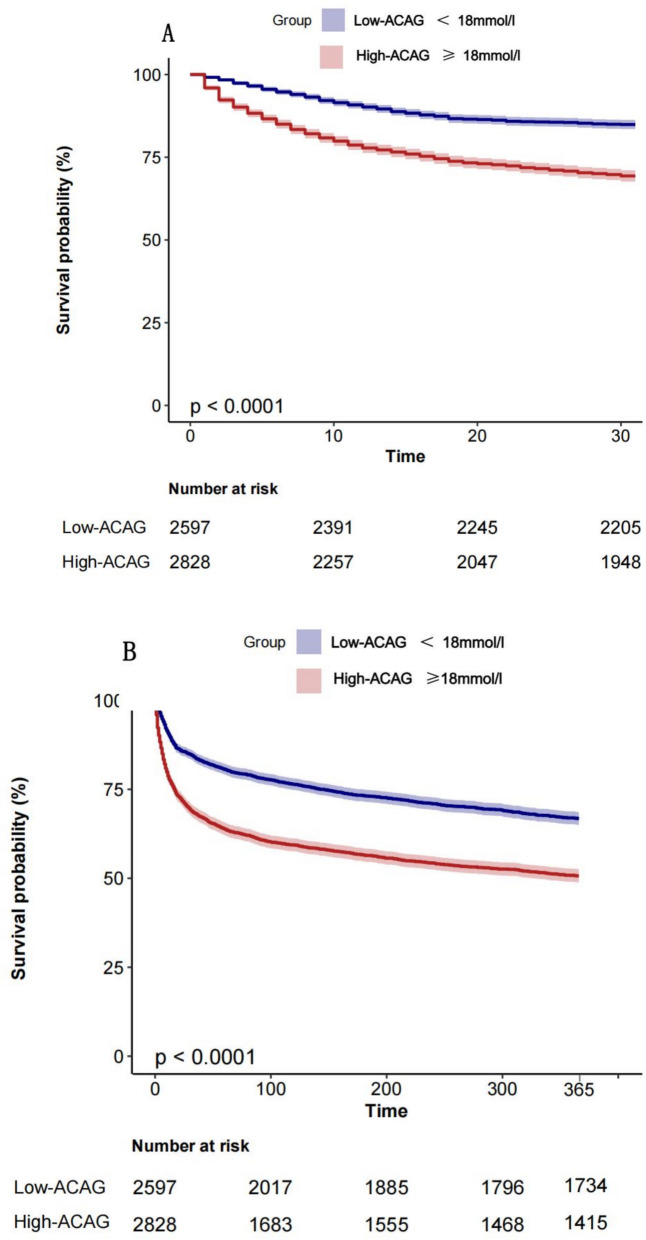
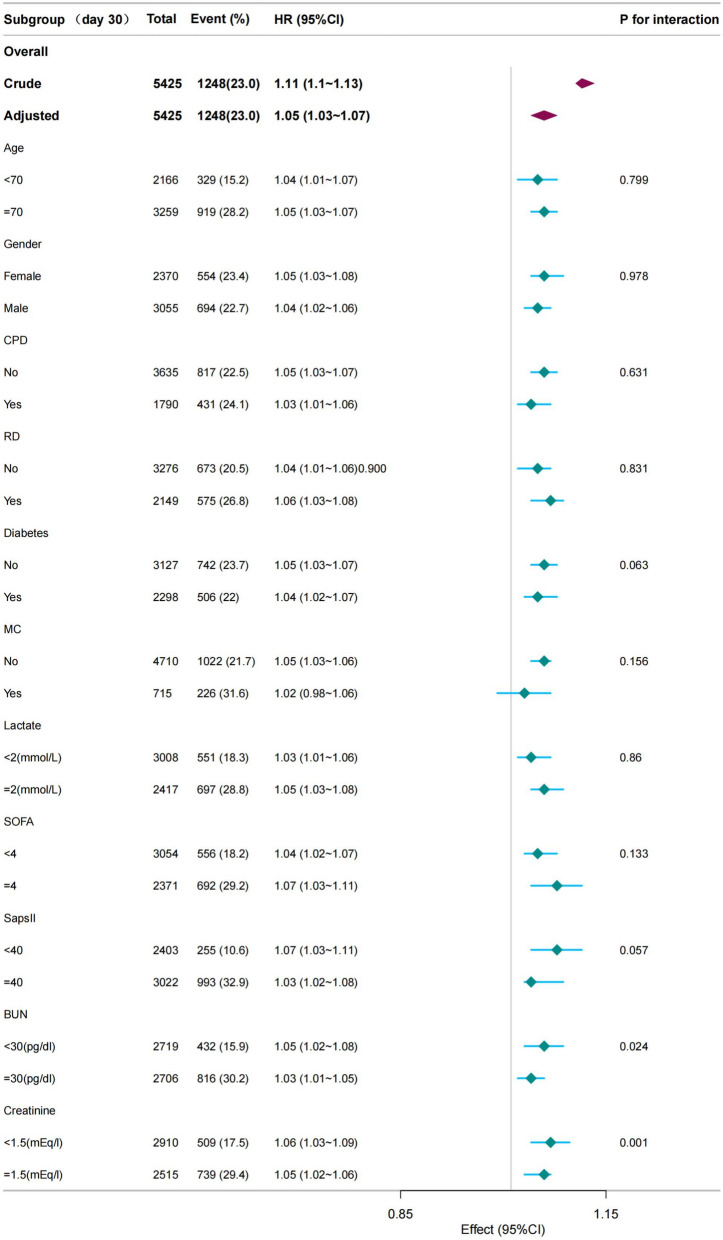
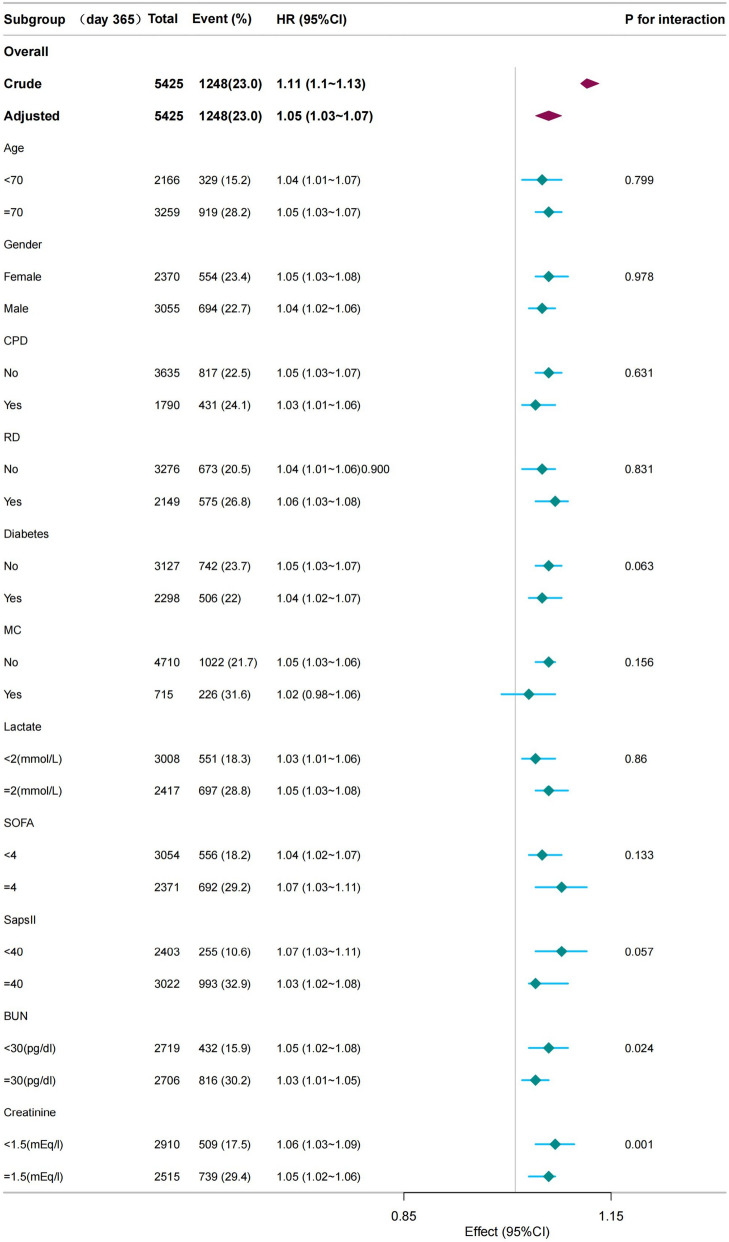
A total of 5425 patients were included in this study. RCS analysis showed a linear relationship between ACAG and mortality (p = 0.075 for nonlinearity). The Kaplan-Meier curve and multivariate Cox regression analysis revealed a positive relationship between ACAG and mortality at both 30 and 365 days post ICU admission. These results were confirmed by subgroup analysis. Mediation analysis showed SAPS II, bicarbonate, BUN, creatinine, hemoglobin, Charlson and ASP III mediated the association between ACAG and all-cause mortality, accounting for 32.34%, - 30.59%, 32.28%, 19.83%, 7.57%, 7.58%, and 25.64% of the mediating effect, respectively (all p values < 0.001). The AUC value for predicting 30-day mortality was 0.643 for ACAG, greater than 0.616 for albumin and 0.604 for AG. For predicting 365-day mortality, the AUC value was 0.641 for ACAG, greater than 0.626 for albumin and 0.597 for AG.
Elevated ACAG is associated with increased mortality in HF patients with AKI, emphasizing the importance of monitoring metabolic parameters in this population. ACAG may be a valuable prognostic marker for HF and AKI. Further research is warranted to determine whether targeted interventions to correct metabolic acidosis could improve outcomes in this vulnerable patient group.
白蛋白校正阴离子间隙(ACAG)升高已被证明与各种危重病的死亡率增加有关;然而,缺乏专门针对并发急性肾损伤(AKI)的心力衰竭(HF)的数据。
从MIMIC-IV数据库中提取并分析2008年至2022年间并发AKI的ICU HF患者的数据。使用多种统计方法评估基线ACAG水平与全因死亡率之间的关联,包括方差膨胀因子分析、受限立方样条(RCS)建模、Kaplan-Meier分析、单变量和多变量Cox回归、亚组分析、中介分析以及受试者工作特征(ROC)曲线分析。
本研究共纳入5425例患者。RCS分析显示ACAG与死亡率之间存在线性关系(非线性p = 0.075)。Kaplan-Meier曲线和多变量Cox回归分析显示,ICU入院后30天和365天时ACAG与死亡率呈正相关。亚组分析证实了这些结果。中介分析显示,序贯器官衰竭评估(SOFA)II、碳酸氢盐、尿素氮、肌酐、血红蛋白、Charlson合并症指数和急性生理和慢性健康状况评分系统(APACHE)III介导了ACAG与全因死亡率之间的关联,分别占中介效应的32.34%、 - 30.59%、32.28%、19.83%、7.57%、7.58%和25.64%(所有p值<0.001)。ACAG预测30天死亡率的AUC值为0.643,高于白蛋白的0.616和阴离子间隙(AG)的0.604。对于预测365天死亡率,ACAG的AUC值为0.641,高于白蛋白的0.626和AG的0.597。
ACAG升高与并发AKI的HF患者死亡率增加有关,强调了在该人群中监测代谢参数的重要性。ACAG可能是HF和AKI的一个有价值的预后标志物。有必要进一步研究以确定纠正代谢性酸中毒的靶向干预措施是否可以改善这一脆弱患者群体的预后。