Bui Tim T, Joseph Karan, Yahanda Alexander T, Vogl Samuel, Ruiz-Cardozo Miguel, Molina Camilo A
Department of Neurosurgery, Washington University School of Medicine in St. Louis, St. Louis, MO 63110, USA.
Department of Orthopedic Surgery, Washington University School of Medicine in St. Louis, St. Louis, MO 63110, USA.
J Clin Med. 2025 Aug 4;14(15):5469. doi: 10.3390/jcm14155469.
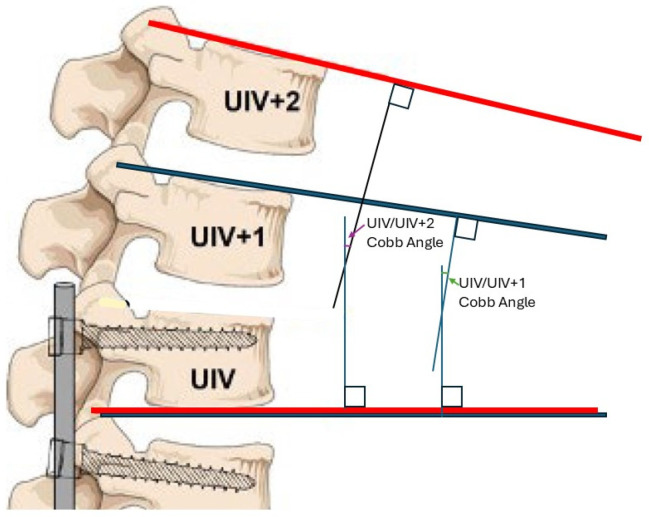
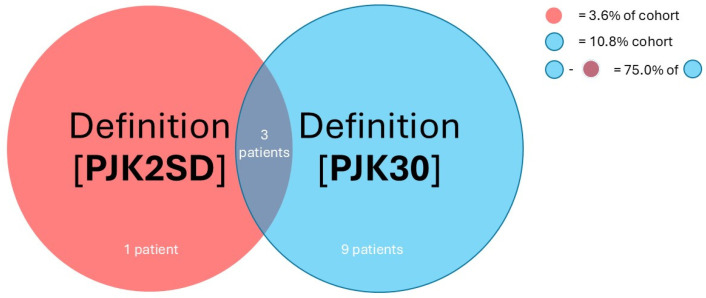
: We sought to characterize the variance and overlap among definitions of Proximal Junctional Kyphosis (PJK) used in the adult spinal deformity (ASD) literature. PJK is defined as excess in PJK angle, a Cobb angle between the upper-instrumented vertebra (UIV) and a supra-adjacent vertebra (SAV), either one (UIV+1) or two (UIV+2) levels rostral of the UIV. No expert consensus exists for threshold angle or which SAV to use. : A total of 116 thoracolumbar fusion patients ≥ 65 years old were reviewed. The UIV+1 and UIV+2 angles were measured. Six definitions of PJK from the literature were evaluated. These definitions were selected based on citation frequency, historical relevance, and accessibility through commonly used databases. Pearson's Chi-squared and pairwise comparisons were performed to evaluate the distinctness and agreement rates among these definitions. : The six definitions of PJK were as follows: PJK angle ≥ 20° with UIV+2 as the (SAV), PJK angle ≥ 10° with a >10° change from pre-op with UIV+2 as the SAV, PJK angle > 2 standard deviations from average with UIV+1 as the SAV, PJK angle ≥ 10° with a >10° change from pre-op with UIV+1 as the SAV, PJK angle > 15° with UIV+1 as the SAV, and PJK angle > 30° with UIV+2 as the SAV, or displaced rod fracture, or reoperation within 2 years for junctional failure, pseudoarthrosis, or rod fracture. [PJK10] and were the most distinct definitions while , , , and showed no significant pairwise differences. [PJK2SD] was stringent, while definition included unique diagnostic information not captured by other definitions. : The use of , , , or is recommended for consistency, with presenting the best balance. Stringent may be beneficial for identifying severe PJK, though with low sensitivity. Overall, PJK definitions must be standardized for the consistent reporting of clinical outcomes and research comparability.
我们试图描述成人脊柱畸形(ASD)文献中使用的近端交界性后凸(PJK)定义之间的差异和重叠情况。PJK定义为PJK角度过大,即上位固定椎(UIV)与上位相邻椎体(SAV)之间的Cobb角,SAV可以是UIV上方一个节段(UIV + 1)或两个节段(UIV + 2)。对于阈值角度或使用哪个SAV尚无专家共识。
共回顾了116例年龄≥65岁的胸腰椎融合患者。测量了UIV + 1和UIV + 2角度。评估了文献中的六种PJK定义。这些定义是根据引用频率、历史相关性以及通过常用数据库的可获取性来选择的。进行了Pearson卡方检验和两两比较,以评估这些定义之间的差异度和一致率。
六种PJK定义如下:以UIV + 2为SAV时,PJK角度≥20°;以UIV + 2为SAV时,PJK角度≥10°且与术前相比变化>10°;以UIV + 1为SAV时,PJK角度大于平均角度2个标准差;以UIV + 1为SAV时,PJK角度≥10°且与术前相比变化>10°;以UIV + 1为SAV时,PJK角度>15°;以UIV + 2为SAV时,PJK角度>30°,或出现移位的棒状骨折,或在2年内因交界性失败、假关节形成或棒状骨折而再次手术。[PJK10]和[PJK2SD]是最具差异的定义,而[PJK10preop]、[PJK15]、[PJK20]和[PJK30]两两之间无显著差异。[PJK2SD]较为严格,而[PJK30]包含了其他定义未涵盖的独特诊断信息。
为保持一致性,建议使用[PJK10]、[PJK10preop]、[PJK15]或[PJK20],其中[PJK10]呈现出最佳平衡。严格的[PJK2SD]可能有助于识别严重的PJK,尽管敏感性较低。总体而言,为了临床结果的一致报告和研究的可比性,PJK定义必须标准化。